
 Over the past week, two respected colleagues sent me links to the Time Magazine article pictured at right seeking my response to the attention-getting title of a new book on ADHD from a behavioral pediatrician in Chicago.
Over the past week, two respected colleagues sent me links to the Time Magazine article pictured at right seeking my response to the attention-getting title of a new book on ADHD from a behavioral pediatrician in Chicago.
While I’ll address some some of the inaccuracies in Dr. Saul’s statements at the end of this post, I was drawn to what I think is a far more interesting question…Given the stigma that exists about the use of medication for ADHD, the difficulty involved in accessing physicians with the knowledge and expertise to properly treat the condition, the cost of doctors’ visits and prescription medication (once-daily ADHD medication can easily cost $2,500 a year or more) and the extraordinary hassles involved with getting insurance companies to pay for what’s needed, why are so many parents pursuing the use of ADHD medication for their children?
In my practice, the vast majority of parents who present seeking my assistance for their kids with ADHD are most fearful about the long-term consequences of their child’s inability to perform in school at the level one would predict from their intelligence and their family’s ability to support their academic success.
Between the kids and families I see in my day job and my current experience as the parent of a bright high school senior entering the final stages of the college selection process upon completion of thirteen years of public education, the stark realities of the world in which our kids are expected to function hit me in the face on a daily basis.
 The volume of academic work kids are expected to produce today substantially exceeds what was expected of students in earlier generations. In 1972, one in 20 high school seniors spent 10 or more hours per week on homework. By 1992, that number increased to one in four. I’ve previously shared this review article examining the research on homework. 80% of U.S. teachers see homework as a tool for teaching organizational skills. According to one study, 82% of U.S. teachers graded homework vs. 14% in Japan and 6% in Germany. A recent study from Stanford University suggests the homework problem may be especially acute at high-performing high schools. As a result, kids with relative weaknesses in organizational skills and the capacity to complete large amounts of work quickly and efficiently operate at a MAJOR disadvantage in academic settings. For many, family life is centered around homework completion. When relationships between kids and parents begin to break down around homework struggles, can parents be blamed for seeking out all possible solutions to the problem?
The volume of academic work kids are expected to produce today substantially exceeds what was expected of students in earlier generations. In 1972, one in 20 high school seniors spent 10 or more hours per week on homework. By 1992, that number increased to one in four. I’ve previously shared this review article examining the research on homework. 80% of U.S. teachers see homework as a tool for teaching organizational skills. According to one study, 82% of U.S. teachers graded homework vs. 14% in Japan and 6% in Germany. A recent study from Stanford University suggests the homework problem may be especially acute at high-performing high schools. As a result, kids with relative weaknesses in organizational skills and the capacity to complete large amounts of work quickly and efficiently operate at a MAJOR disadvantage in academic settings. For many, family life is centered around homework completion. When relationships between kids and parents begin to break down around homework struggles, can parents be blamed for seeking out all possible solutions to the problem?
The competition for slots in desired majors/colleges is markedly more intense than in my generation. Here’s an interesting study examining college admission practices from researchers at Harvard University and the University of Michigan. Here are some key findings…
- The proportion of applicants admitted to elite universities fell by about 25% from 1986 to 2003.
- The likelihood of students being admitted to any college dropped by 9% during that period.
- The percentage of applicants admitted to college with SAT scores below the 25th percentile and 50th percentile experienced the largest drop…by 43% and 23%, respectively.
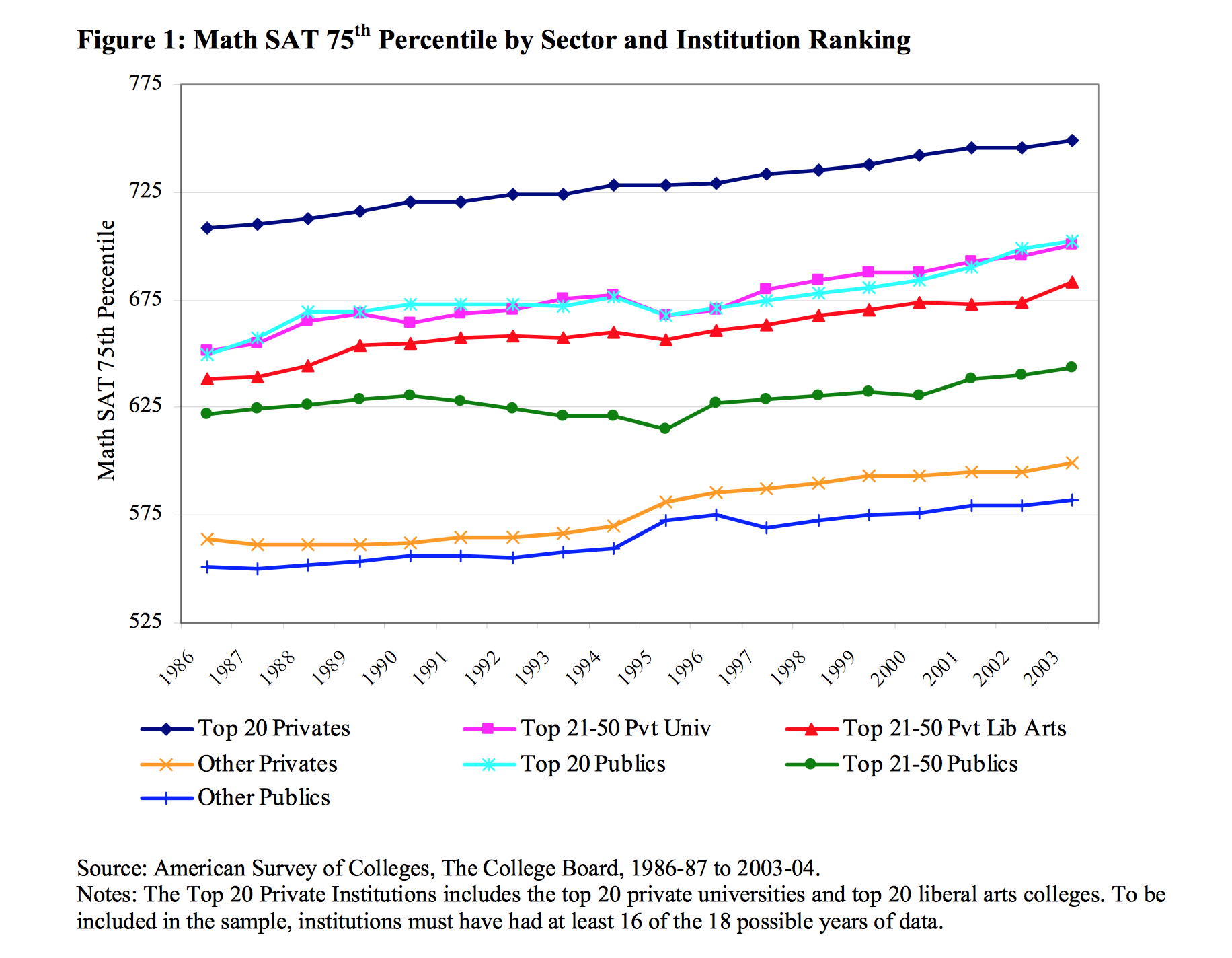
Here’s one graph from the report that demonstrates the increase in competitiveness in college admission, comparing the 75th percentile SAT math scores of students accepted to different types of colleges from 1986 to 2013…
The consequences of suboptimal academic performance are far greater than they were when I was attending school. In 1972, only 29% of high school seniors applied to four year colleges…by 2004, this number increased to 53%. When I graduated from an elite public high school in 1979, a little over 60% of our class went on to college…but for those who did not, blue collar jobs were available in local auto and steel plants that paid solidly middle class wages. In 2012, the median wage for employed high school graduates was $9.50/hour…$2.00 above the Federal poverty line. Only three in ten high school graduates between 2006 and 2011 had found full-time employment by 2012.
 The end result is that the consequences of a lack of success in our educational system can be dire, and if we conceptualize kids having to pass through an ever-increasing number of “round holes” in our schools, the desperation of parents to get their “square peg” through those round holes is mounting. The end result is that parents pursue medication, tutoring, alternative schools and other approaches for their kids who struggle academically because they fear the long-term consequences associated with academic underachievement.
The end result is that the consequences of a lack of success in our educational system can be dire, and if we conceptualize kids having to pass through an ever-increasing number of “round holes” in our schools, the desperation of parents to get their “square peg” through those round holes is mounting. The end result is that parents pursue medication, tutoring, alternative schools and other approaches for their kids who struggle academically because they fear the long-term consequences associated with academic underachievement.
A few thoughts on Dr. Saul’s provocative book title and article…
While I have no doubt that he and/or his literary agent came up with a catchy title that will sell lots of books, his opinion doesn’t appear to be supported by the data. From the American Academy of Child and Adolescent Psychiatry’s Practice Parameters for the Diagnosis and Treatment of ADHD…
Upon reviewing the voluminous literature on ADHD, the American Medical Association’s Council on Scientific Affairs (Goldman et al., 1998) commented, Overall, ADHD is one of the best-researched disorders in medicine, and the overall data on its validity are far more compelling than for many medical conditions. Although scientists and clinicians debate the best way to diagnose and treat ADHD, there is no debate among competent and well- informed health care professionals that ADHD is a valid neurobiological condition that causes significant impairment in those whom it afflicts.
While Dr. Saul is correct in noting that there are lots of other conditions that can produce difficulties with attention, a thorough and detailed evaluation from a competent professional can generally differentiate these conditions from ADHD.
Finally, there is no evidence that large numbers of kids develop tolerance to the effects of stimulants. I’ve seen a few older kids develop tolerance who misused stimulants by dosing their medication to achieve around the clock effects. It’s also possible that some individuals on long-acting stimulants may develop some transient reduction in benefit from accumulating the drug in their system. Most patients who notice such an effect also notice the return of a robust response to medication if they take a brief medication holiday. Kids may occasionally require increases in medication dose as they get older because of increased expectations for academic productivity in middle school and high school. What many describe as “tolerance” is more accurately described as a environmentally-based change in demands upon executive functioning.
We know that lots of kids with relative weaknesses in their capacity to maintain attention when engaged in uninteresting tasks, kids with executive functioning weaknesses and kids with processing speed delays are struggling greatly to cope with the expectations they face on a daily basis in school. While we can all agree that kids who are struggling need a thorough evaluation from a competent professional who takes into consideration all the potential causes of the child’s difficulties, irresponsible statements that help to sell books but shame and blame parents acting out of fear and concern for their child’s well-being aren’t helpful.
***********************************************************************************************************
 Key Ministry has assembled a helpful resource page for church leaders and parents addressing the topic of ADHD and spiritual development. This page includes our blog series on the topic and links to helpful videos and resources for pastors, church staff, volunteers and parents. Access the resource page here.
Key Ministry has assembled a helpful resource page for church leaders and parents addressing the topic of ADHD and spiritual development. This page includes our blog series on the topic and links to helpful videos and resources for pastors, church staff, volunteers and parents. Access the resource page here.





Dr G.
Thanks for this article. Looking forward to meeting you at CLC Network on Thursday. Attached is Oren Mason’s response to Dr. Saul’s Time article. See you soon. Doug Bouman
LikeLike
I don’t mean this to be meanly critical, but as a ministry, are you supposed to support fear-based actions? Remember: “For God has not given us a spirit of fear and timidity, but of power, love, and self-discipline.”
Your article is suggestive of one thing that can be summed down to one question:
How do you make your children fit into the box?
The answer:
You get them out of the box.
Where’s your peace? There’s your answer.
LikeLike
Hi Gaynell,
Thanks for your comments.
What I was describing here wasn’t meant to be an endorsement of the approach many families are pursuing. It’s important to keep in mind that God loves our kids and has a plan or a purpose in mind for them. But it’s also important when folks look at this issue to understand that what is being expected of kids in terms in terms of academic performance is quantitatively and qualitatively different now when compared to 20 or 25 years, and the alternatives for making a reasonable living far more limited for kids who aren’t able to successfully navigate the educational system.
When families come through our practice who are struggling with this issue, we frequently talk about solutions that involve “getting them out of the box.” In our area, we have a private, secular school that has sought to establish a learning environment and teaching style most favorable to kids with attention and/or learning differences. I’ve had some families successfully employ home-schooling approaches. But not everyone has the resources to pursue those types of approaches.
By the time these kids get to us, there has frequently been significant disruption to family relationships because of homework and school pressure. From a developmental perspective, I think it’s essential that parents maintain their relationship with their child or teen because without that relationship, the parent has little ability to influence their child’s faith development. I’d also be interested to hear what your youth pastor might say if you were to ask them whether they think the volume of work expected of kids in school negatively impacts church attendance, youth group participation and involvement in service activities.
LikeLike
How about this article? Consumer Advertisements of Psychostimulants: A Long Record of Misleading Promotion
In 2005, we wrote to the FDA regarding a perceived disconnect between widespread DTCA for attention-deficit/hyperactivity disorder (ADHD) medications and the peer-reviewed scientific literature. Such a disconnect is important because FDA regulations require that DTCA be consistent with the FDA-approved product label. The FDA notified us that it would further evaluate our concerns, but the advertisements continued. Three years later (on September 26, 2008), the FDA issued letters to pharmaceutical companies that sell psychostimulants (eg, methylphenidate and mixed amphetamine salts), warning them to cease misleading promotion — including advertisements to both prescribers and consumers. The warning letters state that among other alleged infractions, the targeted advertisements overstate the efficacy of psychostimulants. Some might question the delay in regulatory response. However, our central question is, where has the mainstream medical community been over the past 3 years while — as the FDA has now acknowledged — Americans were being misled about psychiatric drugs for children?
As anyone familiar with the treatment of children with an ADHD diagnosis already knows, psychostimulant medications represent but one type of intervention used with this population and are by no means a “magic bullet” treatment. Both the evidence-based literature and even the prescribing labels for psychostimulants acknowledge the need for a comprehensive treatment program in the treatment of ADHD. There is also a paucity of research demonstrating that the prescription of stimulants predictably results in enhanced socioemotional development.
Therefore, when we wrote to the FDA in 2005, we were concerned about a highly visible US advertising campaign for Adderall that featured smiling children and their parents. The advertisements were widely distributed in popular periodicals, such as People magazine, and they claimed that Adderall was a “trusted solution for ADHD” that would lead to “friends that ask him to join the group” and a “family hour that lasts for hours.” The Web site featured a celebrity endorsement by television personality Ty Pennington, in which he claimed that Adderall did not affect his appetite or sleep. All of these advertising claims exaggerated the positive impact of this medication as measured by scientific evidence. For instance, academic difficulties are often a precipitating factor in the diagnosis and treatment of ADHD, and thus parents may find claims that psychostimulants increase academic performance particularly compelling.
For years, Adderall advertisements have used the slogan, “Schoolwork that matches his intelligence.” In 2005, we wrote to Shire Pharmaceuticals regarding this claim, pointing out that the experimental evidence was limited to improvement on a 10-minute math test, and questioning whether this was equivalent to the more global concept of “schoolwork.” At the time, Shire defended its advertising campaign. The FDA has subsequently clamped down on the gap between peer-reviewed scientific evidence and such claims, noting that an improvement on ADHD measures does not necessarily correlate with improved academic outcomes, and warning Shire directly that “improvement in attention, as evidenced by increased numbers of math problems answered correctly, has not been correlated with an improvement in academic performance throughout the day, an end point which has not been studied.”
This chain of events raises several important issues. First, we wonder how many parents have been “driven to the doctor” and made the difficult decision to medicate their child under the influence of misleading advertising. However, there is a larger problem. There were few (if any) dissenting voices raised from rank-and-file academic psychiatrists who objected to these misleading advertisements. How is it that over the past 3 years, we have not seen strong public objections to the widespread dissemination of obviously inaccurate information? Beyond academia, practicing child psychiatrists and pediatricians who treat patients with ADHD must also be aware of the disconnect between these highly visible advertisements and the scientific evidence.
While we have focused here on Adderall, for years we have also noted questionable promotional materials for several other ADHD medications. Yet, the voice of mainstream practicing and academic psychiatrists has seemingly been silent. Why? It is easy — perhaps too easy — to blame the FDA for inefficient regulation, but at least the agency has finally acted. This is in stark contrast to the many professional societies and representative bodies made up of physicians who study ADHD or who treat affected patients, from which we have seen no public objections. Certainly, a public outcry from prominent academic psychiatrists could have influenced the FDA to act sooner. Is it possible that the flow of money from the pharmaceutical companies to influential academic psychiatrists (a situation now being investigated by Congress) has brought with it a certain willingness to remain silent?
A recent study found that stimulants are prescribed at a rate 3 times higher for children in the United States than for their counterparts in Germany and the Netherlands. According to the researchers, DTCA is one likely reason for the higher rate of drug use in the United States. Obviously, advertisements that exaggerate the efficacy of stimulants are intended to increase sales, and therefore, the rate at which we medicate our children.
Children with behavioral disorders are a vulnerable population. Certainly, their welfare — and the science behind our efforts to help — should come before commercial interests. The policies, practices, and advocacy of the medical profession should clearly demonstrate a preference for evidence-based information over commercial advertising.
Jonathan Leo, Ph.D. / Jeffrey Lacasse, Ph.D.Jonathan Leo, Ph.D. / Jeffrey Lacasse, Ph.D.
LikeLike