
 Welcome to our Summer 2013 blog series…Ten Questions Parents and Caregivers Ask About Kids and Medication. Today, we’ll kick off the series by examining the question Why Does it Seem So Many Kids Are On Medication?
Welcome to our Summer 2013 blog series…Ten Questions Parents and Caregivers Ask About Kids and Medication. Today, we’ll kick off the series by examining the question Why Does it Seem So Many Kids Are On Medication?
Let’s start with a look at some data examining prescribing practices with psychoactive medication and kids…
Here’s data from the U.S. Centers for Disease Control looking at the percentage of U.S. kids between ages 8 and 15 prescribed medication across a range of mental health conditions:

From the Wall Street Journal…

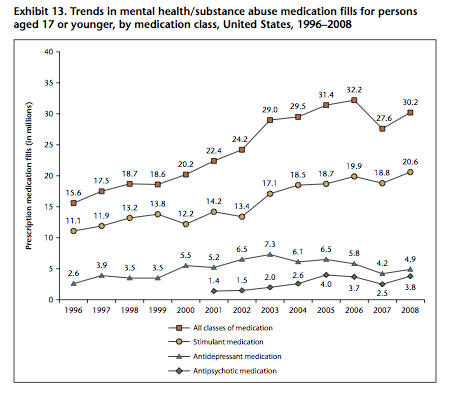
From the U.S. Substance Abuse and Mental Health Services Administration (SAMSHA):
Getting back to our original question…Why does it seem so many kids are on medication?
ADHD is (by a very large margin) the mental health condition for which medication is most frequently prescribed. But the number of kids taking medication for ADHD on any given day may be dramatically overstated. Looking at the statistic above, 8.6% of kids ages 8-15 received at least one prescription for ADHD medication in 2008. In 2009, according to SAMSHA statistics, 5.29 million kids ages 17 and under received prescriptions for stimulant medications. If we use SAMSHA’s data for the number of prescriptions written in 2008 (one year earlier) and divide by the number of kids with ADHD, the typical kid with ADHD receives approximately four prescriptions per year for a thirty day supply of medication. Here’s an earlier blog post that explains why the number of prescriptions filled for ADHD is far lower than expected.
The success of available treatments have created a culture in which medication has become more accepted. Social networks likely play a significant role in parents’ willingness to consider medication. We see this in our practice…When several kids with well-connected parents respond positively to medication, it’s not at all unusual for us to see a steady stream of families from that school seeking help.
Parents who themselves have responded to psychiatric medication are more accepting of having medication prescribed for their children. We see this most often when we’re considering medication for a kid with anxiety or depression. When mom or dad has responded positively to medication, the child is more likely to be started on medication, especially if some type of counseling/therapy has previously been tried. The converse is often true with ADHD medication…parents seek out evaluation after observing a positive response to medication in their child.
Parents aren’t necessarily willing (or capable) of implementing behavioral, home-based interventions. The apple often doesn’t fall far from the tree. Kids who struggle with prioritization, self-control and a lack of follow-through frequently have parents who share the same struggles. For parents who are willing to implement behavioral approaches, good help may be nearly impossible to find. We’re fortunate to have a capable practitioner in our area with a team that offers home-based behavior intervention at a reasonable price. Mental health benefits offered under traditional health insurance doesn’t typically cover home-based behavioral therapy, or administrative demands are so arduous that the few service providers available choose not to contract with insurance.
Medication often serves as a substitute for effective evidence based psychotherapies in both public and private settings. Good psychologists, counselors and social workers are very hard to find! Pediatricians and family physicians are generally available in areas where mental health resources are in short supply. Here’s a chart review study presented this past May from the American Academy of Pediatrics reporting 9% of kids in 14 sites representing 11 states received medication from their pediatrician between 2009 and 2011.
The ever-increasing demands for academic productivity from schools accompanied by the rapidly escalating cost of higher education have led more families to seek out treatment for ADHD, and contribute to the increased prevalence of anxiety in teens. In my 22 years in practice after completing my fellowship, one of the most striking changes I’ve seen is the increase in the volume of work kids are assigned in school, along with increased expectations from both schools and parents for kids to manage and organize their workloads. Declining grades related to missing homework might be the most common concern I see on referrals of new kids to our practice. The pressure for good grades and high SAT/ACT scores kids experience from their parents…and themselves can be overwhelming…as evidenced by the article featured in this commentary.
Training bias on the part of practitioners. For nearly all of the residents and fellows who pass through our practice, much of their clinical training takes place in very busy community mental health centers where trainees are expected to evaluate and treat lots of kids in relatively brief time slots…and focus almost entirely upon medication needs. Young psychiatrists who graduate from training do what they’re trained to do when they move into public or private mental health positions.
Reimbursement bias on the part of the government and commercial insurers. The CPT codes physicians, hospitals and clinics are required to use in billing for services heavily favor medication services compared to psychotherapy or other psychosocial interventions. Under the new codes (effective January 1, 2013), the discrepancy in compensation for medical services vs. psychotherapy is more pronounced than in the past, and the greater the complexity of the child’s medication regimen (and required medical decision-making), the easier it is to qualify for billing codes linked to higher reimbursement.
The impact of cultural change on our kids. 41% of U.S. children born in 2010 come from single parent homes…homes where kids are five times more likely to be raised in poverty. Between school and scheduled activities, modern kids have far less time to play. Kids are impacted when marriages end in divorce. We know that kids who have been exposed to chronic stress from neglect, physical, sexual or emotional abuse or violence in the home are at risk of changes in brain development associated with suicide attempts and depression.
Should we be surprised so many kids are prescribed medication given what we know about the design of our mental health care delivery systems, our expectations for academic performance, the breakdown of so many families and the values of our culture? I think not.
***********************************************************************************************************
 Key Ministry offers a resource center on ADHD, including helpful links, video and a blog series on the impact of ADHD upon spiritual development in kids and teens. Check it out today and share the link with others caring for children and youth with ADHD.
Key Ministry offers a resource center on ADHD, including helpful links, video and a blog series on the impact of ADHD upon spiritual development in kids and teens. Check it out today and share the link with others caring for children and youth with ADHD.





I almost dreaded reading this because I was afraid you’d be heavily weighted on the side of not medicating children…which seems to be the new trend. I think your assessment was very fair and made me see things in some new ways. In our case, our daughter responded so positively to medication that I can’t help but resent those who prevented us from accessing it for so long. The difference was night and day – a girl who was running away from home, being self-destructive, violent and profane – transformed over the course of a couple of weeks into a girl who is polite, cooperative, obedient and even happy.
I do think you underestimate the difference between insurance reimbursement for therapy versus medication. Good and appropriate therapy (in our case for issues related to early trauma) IS nearly impossible to find – but once we found it, we had to manage to pay for it entirely out of pocket. Our insurance has no coverage for mental health care apart from partial coverage of a few psychiatrist visits. In order to get the care she needed our daughter had to be assessed as severely mentally disabled so she could be put on Medicaid. I have no idea how this will impact her future – but since therapy is very helpful for her, it had to be done.
LikeLike
Hi Annie,
Thanks for your interest in the blog!
I fully appreciate how difficult it is for parents to access excellent therapy at any price. For the last eighteen years I’ve run a group practice…we have an extraordinarily hard time finding therapists with the necessary skills to join our practice. It’s very difficult for us to find therapists in other practices who we’re comfortable referring families to, and when we do, their practices tend to fill very quickly.
Keep reading…and commenting!
LikeLike