A couple of weeks ago, I had the opportunity to speak with with Stephanie Prosser and Sara Collins of Reach For A Difference in Abilene, TX. Reach for a Difference exists to support individual, family & community actions to address identified needs and issues of persons with autism spectrum disorders and other developmental delays in the West Central Texas area surrounding Abilene. Stephanie and Sara had contacted us because they were working with the West Central Texas Council of Governments and the Texas Council for Developmental Disabilities on a program to help those with special needs and their families find an inclusive church home, and to encourage faith based organizations to promote inclusion.
A couple of weeks ago, I had the opportunity to speak with with Stephanie Prosser and Sara Collins of Reach For A Difference in Abilene, TX. Reach for a Difference exists to support individual, family & community actions to address identified needs and issues of persons with autism spectrum disorders and other developmental delays in the West Central Texas area surrounding Abilene. Stephanie and Sara had contacted us because they were working with the West Central Texas Council of Governments and the Texas Council for Developmental Disabilities on a program to help those with special needs and their families find an inclusive church home, and to encourage faith based organizations to promote inclusion.
This past Tuesday (the day after we offered a training in Northeast Ohio attended by representatives of eleven different churches), Stephanie’s organization offered a symposium titled Bridging the Gap to link families impacted by disabilities and faith-based organizations in Abilene. The event was considered a “great success” because of the large turnout. But in contrast to our event this past Monday, the turnout in Abilene was “all disability organizations and little to no churches.”
Stephanie offered to share her family’s story with our readers. It serves as a stark reminder that while great strides are being made in opening more churches to families of kids with special medical, behavioral, emotional and developmental needs, there continue to be cities of substantial size here in the U.S. where families impacted by disability have nowhere to go on Sunday mornings if they wish to worship as a family. Here’s Stephanie…
It’s a weird world this Autism world that our little family has now embraced as our own!
As Christian parents we know the importance of spirituality in our lives, of connection and of growth. As autism parents we also know the importance of safety, patience, routine, and experimentation. My husband (Timothy) is 37 and has only in the past two years found out that he is on the spectrum, along with our four year old son, Sebastian. We discovered Timothy’s diagnosis through genetic testing while going through the process of finding our son’s diagnosis. This new information explained a lot while leaving much needing to be explained. It gave us answers without solutions, opened many doors to us, and seemed to close just as many. It was an unknown world in which the only thing we knew for certain was that it was going to affect many things in our lives, and we were going to have to make many changes.
We have always been connected to the church somehow through our entire lives. My parents were routine churchgoers, my father studied ministry, and my mother served in various departments in the church. My husband’s parents are missionaries, both as preachers and evangelists. My husband went to Christ of the Nations Bible College and received his degree in ministry. He then went on to work on his church’s production team.
On my end while growing up, my family had grown apart from the church and I stepped away for some time, but like Joseph I made my way back for my prodigal return. When my husband and I became a couple one of the things we most enjoyed together was attending service. His faith and obedience to the Lord was what attracted me to him when we first met, and still does!
It was exciting doing church together as a new couple, laying a foundation for our marriage, and growing close to God and each other. We had a few glitches in first finding a church home, but in the end we found our niche, and had found a church family to call our own.
After a year, we were pregnant and that imposed some stress on our church life. It’s so much easier to hit the snooze button than to try to button up your jeans and waddle into a room full of uncomfortable pews while eight months pregnant! After Sebastian was born, we’d drag him into church with 40 pounds of baby gear, including my breast pump and I’d spend most of my time in the seclusion of the wet nursery feeding my child and listening to the sermon through the overhead intercom. My husband and I missed one another in that environment, getting to share Jesus together. We were young but we were exhausted. Going to church was becoming a chore, and we were ready for Sebastian to grow up just enough to go into the regular nursery so we could be reunited!
Well, our son grew up, but our idea of being together in a church service was slowly being pushed out of the window. As my son grew from baby to toddler he became harder to please and was more work for the church volunteers. He was prone to crying or screaming, and didn’t have any interest in the activities the other kids were doing. He was clingy and hard to drop off. We couldn’t get through more than a few minutes of service before my husband and I became tag team babysitters. We never enjoyed a service together. I began resenting the process of going to church.
We struggled to get to church on time, and opted for separate cars, in lieu of arguing the whole way to the chapel. We’d get frustrated with our son for not being more like the other kids. We would get frustrated at one another for not listening well enough to tell the other what happened while they were gone! We’d get frustrated at the church staff for the minute reasons we were being paged over and over again. Our son was throwing tantrums and we were throwing tantrums right there beside him! It became too much for us, so we began to “church shop” for the holy grail of churches in our community that would be able to care for our son and allow us to get through a solid service! We figured it shouldn’t be that hard. We were familiar with people in many churches and were a part of church circles. We live in the Bible Belt and Abilene is the church capital of our State and possibly the nation. Finding a place to go to church should not be an issue…and it wasn’t! Finding a place to stay WAS.
We were getting similar results in all of the churches we went to. So we began to settle for churches that didn’t really meet our spiritual needs but met our son’s needs. We found a very small church two minutes away from our home. It’s population was largely adults over the age of 60 and there were very few (if any) kids on Sunday. The classrooms weren’t very well-decorated or furnished, the atmosphere was quiet and the children’s areas were well-staffed. It was perfect for Sebastian and not so great for us. We were missing the connection.
But all things happen for a reason and work for good for those who love Christ Jesus! At this little church, my son was able to get through a service in the children’s church and that made us happy. Sebastian loved to go, and would even ask to go on weekdays. He began to pester us about church! “When is it church time?” was the song that played like a broken record from my kid’s lips, over and over. It was easy to find solace in that for a while because as a mother, one of the things that I want to ensure most is that my child is raised around a spiritual atmosphere. He will need those roots as he grows older and steps out into adulthood. I want him to have that foundational opportunity and experience. So his enthusiasm became my enthusiasm!
It ended up being a very fleeting form of enthusiasm. As we just “attended” church successfully, I could tell our spirits were dwindling. The more my husband steps away from church the more “lost” he appears in his eyes and in his decision making and I became more fearful and woeful. This is not a state I like to be in, and through some of the complacency haze I could see that we were going the easy route via our new excuse- “autism”. We both longed for more and wanted more for our family. This posed a new question-How? How are we going to do this? In the back of my mind I thought to myself, “Please do not let this be a series of bad experiences for my child.” I don’t want to see him hurt, and I definitely do not want to see his attitude change toward going to church!
Around that time we had the privilege of getting away via an out of town car trip to film as our friend Pastor Brandon become consecrated as a bishop. We stayed the weekend and were visitors at his church service and in his home. Church went wonderfully. The volunteers were very open to hearing about and adapting for our son’s disability. Their attitudes towards us were glowing and their compassion for my son was genuine. After dining with the bishop and gleaning some of his wisdom, we vowed to return to an old church that we had loved but where Sebastian had a difficult time.
There are many things that went into us returning to one of the churches we had attended for some time. Sebastian was now older and had gone through a year of extensive therapy (speech, behavioral, occupational, physical, and food therapies). He was also enrolled in a special education program at school and had adjusted to the classroom experience. The church had changed. Volunteers and the new leaders were familiar with the special needs world; there were other autistic children in Children’s church and Sebastian is high-functioning. His needs aren’t as great or his behavior as disruptive as other children. We had some plusses on our side in attending. We had also changed. We were more familiar with our son’s disability and what made him tick. We were more vocal about his needs, and more able to help instead of “babysitting”. We opened up communication, allowing us and the church to work together. We had grown and while we were gone, the church had too!
This was a perfect return for us, but not without snags. Sebastian has left church several times injured. Not a new thing for us. He’s clumsy and accident-prone. Probably not new to the church, but I could see the fear in the eyes of the volunteers as they hand over our injured boy! It’s a process. We are all learning and growing through the experience. Growth is always a good thing!
While going through the process of learning, accepting, and embracing my child’s disability, I became an advocate and leader of a local non-profit called REACH for a Difference, The Autism Spectrum Partnership Network here in Abilene. We connect persons on the spectrum and their families with resources in the community and create programs to fill in the gaps where families’ needs are not being met. We are currently working with another disability organization in Abilene on a program to promote inclusion in our area churches. We are “Bridging the Gap” between those with disabilities and our local faith based organizations. Our program promotes education, awareness, inclusion, and the empowerment of people with disabilities within the church. We want to see people with disabilities not only be able to attend church, but to plug in and grow. We want to see friendships built, communication paths opened, people serving, and people finding a home away from home. I have met many families through this program with experiences similar to mine and many more who have been asked to leave a church or turned away from a church because of their disability. We have made it our mission help build the necessary bridge that it will take so that no one is turned away from the church and ultimately away from God.
I was ecstatic to discover Key Ministry! I am excited that there is a program already in existence doing this great work and thankful to them for taking the time to Skype with our organization. With the information they gave us and the great example Key Ministry has set, I know that we can be a success story as well!
***********************************************************************************************************
 Key Ministry has assembled a helpful resource on the topic of Asperger’s Disorder and Spiritual Development. This page includes the blog series Dr. Grcevich and Mike Woods developed for Key Ministry, links to lots of helpful resources from other like-minded organizations, and Dr. Grcevich’s presentation on the topic from the 2012 Children’s Ministry Web Summit. Click here to access the page!
Key Ministry has assembled a helpful resource on the topic of Asperger’s Disorder and Spiritual Development. This page includes the blog series Dr. Grcevich and Mike Woods developed for Key Ministry, links to lots of helpful resources from other like-minded organizations, and Dr. Grcevich’s presentation on the topic from the 2012 Children’s Ministry Web Summit. Click here to access the page!
0.000000
0.000000

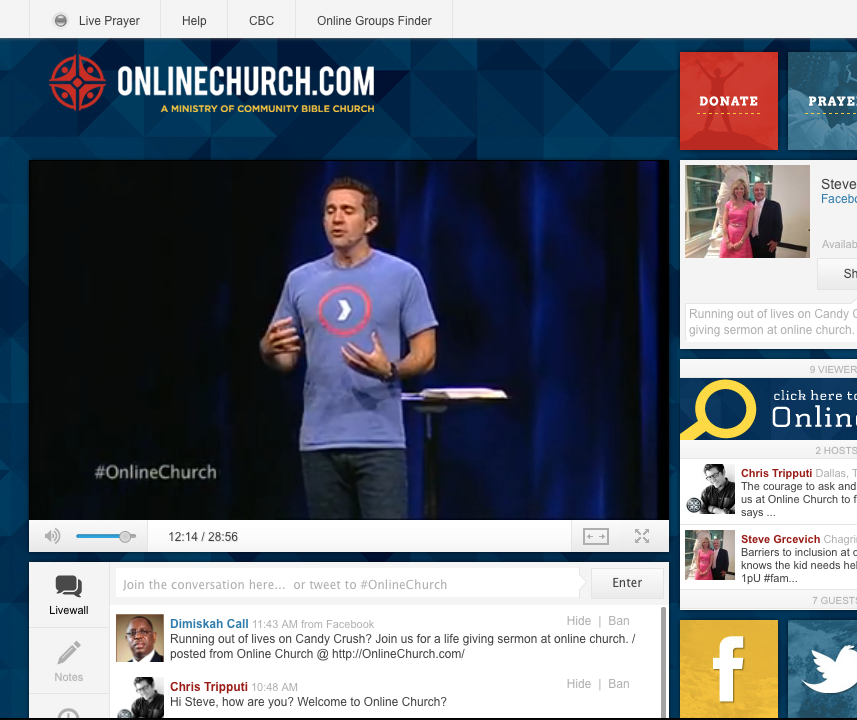
 Please join us on Thursday, March 6 for our first Inclusion Fusion Web Symposium as Nils Smith and I discuss the topic… Is Online Christian Community Really Community. The interview with Nils was prerecorded and will be available every hour on the hour from 7:00 AM Eastern Time on Thursday until midnight Eastern Time on Friday. Nils will be available for an interactive chat from 12:00 PM-2:00 PM Eastern (11:00 AM-1:00 PM Central) and from 9:00 PM-10:00 PM Eastern (8:00 PM Central, 6:00 PM Pacific). We’re going to be talking about his experiences as an online church pastor, and initiating a lively discussion about how online church campuses might be used as a tool for local churches to reach out into their local communities to make connections with families impacted by disabilities.
Please join us on Thursday, March 6 for our first Inclusion Fusion Web Symposium as Nils Smith and I discuss the topic… Is Online Christian Community Really Community. The interview with Nils was prerecorded and will be available every hour on the hour from 7:00 AM Eastern Time on Thursday until midnight Eastern Time on Friday. Nils will be available for an interactive chat from 12:00 PM-2:00 PM Eastern (11:00 AM-1:00 PM Central) and from 9:00 PM-10:00 PM Eastern (8:00 PM Central, 6:00 PM Pacific). We’re going to be talking about his experiences as an online church pastor, and initiating a lively discussion about how online church campuses might be used as a tool for local churches to reach out into their local communities to make connections with families impacted by disabilities. We’re very blessed to have Nils join us for this conversation! He truly is among the world’s leading experts in online church experiences. His wisdom and expertise is sought out by churches nearly everyone would recognize, and his experience in serving Life Without Limbs affords him a unique perspective on the application of technology in disability ministry.
We’re very blessed to have Nils join us for this conversation! He truly is among the world’s leading experts in online church experiences. His wisdom and expertise is sought out by churches nearly everyone would recognize, and his experience in serving Life Without Limbs affords him a unique perspective on the application of technology in disability ministry.