
 The National Center for Health Statistics issued a stunning report ten days ago examining suicide rates in the U.S. over the period from 1999 to 2014. Across the board, increases in rates of completed suicide were noted in men and women of all ages. The most striking increases were observed among 10-14 year old girls. Among males, the largest percentage increase in completed suicide was seen among 10-14 year old boys.
The National Center for Health Statistics issued a stunning report ten days ago examining suicide rates in the U.S. over the period from 1999 to 2014. Across the board, increases in rates of completed suicide were noted in men and women of all ages. The most striking increases were observed among 10-14 year old girls. Among males, the largest percentage increase in completed suicide was seen among 10-14 year old boys.
Here’s a summary of the key findings. For more, you can read the entire article from the U.S. Centers for Disease Control here…
From 1999 through 2014, the age-adjusted suicide rate in the United States increased 24%, from 10.5 to 13.0 per 100,000 population, with the pace of increase greater after 2006.
From 1999 through 2014, the percent increase in the age-adjusted suicide rate was greater for females (45% increase) than males (16% increase), resulting in a narrowing of the gender gap in suicide rates (as measured by rate ratios).
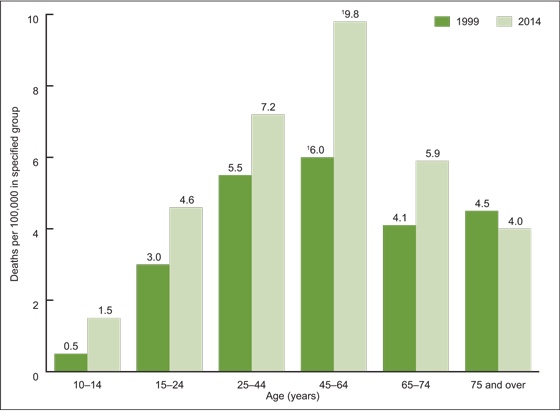
Although based on a small number of suicides compared with other age groups (150 in 2014), the suicide rate for females aged 10–14 had the largest percent increase (200%) during the time period, tripling from 0.5 per 100,000 in 1999 to 1.5 in 2014.
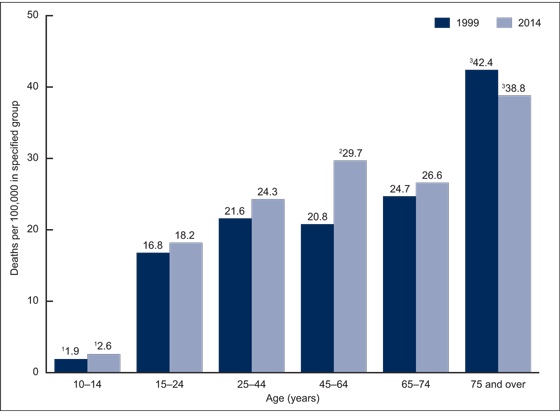
While males aged 10–14 had the lowest suicide rate of all age groups (among males), this group experienced the second-largest percent increase (37%) from 1999 through 2014 (from 1.9 to 2.6).
Suicide rates for females, by age: United States, 1999 and 2014 Source: NCHS, National Vital Statistics System, Mortality.
Suicide rates for males, by age: United States, 1999 and 2014 Source: NCHS, National Vital Statistics System, Mortality.
What the statistics don’t tell us is WHY we’re seeing such a significant increase in the rates of suicide among children, teens and young adults, along with sizable increases in suicide rates among adults of middle age, especially women. What might be causing the increase? I’d like to put forth a few “educated guesses.”
The pressure to succeed. The pressure operates on so many levels. Teachers and schools are under great pressure for kids to perform well on standardized tests. My all-time productivity record for time spent with kids in our practice was the two weeks prior to the first Common Core testing. Parents put pressure on their kids to succeed academically because many need their kids to qualify for substantial scholarships in order to help with the outrageous cost of a college education. They also put pressure on their kids to do well academically because higher education is increasingly necessary for the types of jobs that will enable them to generate a stable income sufficient to support a family. Kids put immense pressure on themselves to do well in school. All too frequently, a poor test result is viewed as a cataclysmic event by the kids I see.
We deny our kids opportunities to develop resiliency. I appreciate the initiatives and programs done in our schools to prevent bullying because the effects of bullying are especially severe for the kinds of kids we see in our practice. While we’re teaching kids not to bully others, we also need to be teaching them how to deal with adversity. In a pluralistic society, our kids are going to encounter people with whom they will intensely disagree. In our efforts to protect kids against emotional hurt and failure, we all too often have left them without the mental and emotional tools to overcome the setbacks or conflict that are inevitable later in life.
My high school junior expressed an interest in taking a visit to Emory University the week before this happened. In my humble opinion, the extent to which college administrators enable the kids within their learning communities to function as emotional invalids borders on criminal negligence. When we teach our kids that they can’t function outside of “safe spaces,” we end up with this…
I feel bad for the kid in this video. How does one cope with the demands of live with the capacity for emotional self-regulation of a two year-old? “Snowflakes” don’t do very well when the heat gets turned up.
When parents continually rescue their kids from the consequences of their own failures, they go away to college without the life skills to interface with professors when they have a setback or the study skills and self-discipline to overcome a poor grade. I see this time and time again in my practice…children of parents who are calling the principal or headmaster every time their kid has a conflict with a teacher crash and burn when the inevitable challenges hit after they go away to college.
The impact of social media. A common thread among conditions that contribute to the overall sense of hopelessness that all too often leads to suicidal thoughts and behavior (anxiety, OCD, depression) is the propensity for an unrealistically negative view of oneself. Social media radically expands the opportunity for kids and adults to experience despair through exposure to video, images and text with the potential to shatter the already fragile self-images of all too many children, teens and adults.
You’re a girl in middle school who feels unpopular…not only can you now see the “popular” kids from school having fun with one another on Instagram, but you can measure your relative lack of popularity by comparing the number of followers you have against theirs. No one asked you to the prom? You now have the opportunity to see the boy you hoped to dance with at the prom enjoying himself with someone else thanks to Vine and Snapchat. Stuck in a dead-end job and struggling financially? Check out the pictures your neighbors and old friends from high school are posting online of their exotic vacations. Feel inadequate as a parent? It’s pretty hard to watch the “brag fest” on Facebook as parents post the scholarship offers their kids have earned and admission letters to prestigious colleges while your kid is looking forward to community college and a part-time job.
 A culture in which sexual liberty is a dominant value and sexual expression is central to identity. There aren’t a lot of sexual taboos remaining in our culture and the taboos that remain are quickly disappearing. And a lot of people are getting hurt as a result…some, fatally.
A culture in which sexual liberty is a dominant value and sexual expression is central to identity. There aren’t a lot of sexual taboos remaining in our culture and the taboos that remain are quickly disappearing. And a lot of people are getting hurt as a result…some, fatally.
Teaching from the New Testament regarding sexual behavior isn’t there because God’s a prude or some heavenly killjoy. God invented sex. Sex in his creation was (and is) intended for good. The rules about sex are lovingly given to us for our own protection.
From a mental health perspective, some people need rules governing their sexual behavior more than others do. This is an issue I see with the kids in my practice all the time. I wrote at length here about the data linking sexual relationships to suicide risk in teens. I see this impacting kids…and their parents in other ways. The folks who shape our culture…people in entertainment, education, the media, sports – may have the money or resources to mitigate the consequences of their pursuit of sexual freedom. Jennifer Garner’s kids aren’t going to find themselves in poverty or having to change schools after their father (allegedly) had a fling with their nanny. But the same may not be true when dad makes $17/hour working in a factory and runs off with a co-worker.
What do you do when you’re emotionally fragile and the person with whom you’re intimate leaves you for someone else? What do you do when you’re a ninth grader in a culture that values physical attractiveness when you’re not very attractive? Or when your parent invites a serial abuser into your home because they’re desperate for a relationship to help them fill the emptiness they experience? Or a woman who has developed an identity around her attractiveness when the inevitable changes associated with the aging process start to take hold? From where do you derive your hope in a better future as time takes its toll?

Percent distribution of the 10 leading causes of death, by age group: United States, 2013
While we need more mental health professionals and more effective treatments for depression and professionals with better training to recognize the signs associated with suicidal behavior, the increase in suicide we’ve seen in recent years, especially acute over the last ten years are more a sign of a sick society than anything else. Suicide is (again, after dropping to #3 in the first few years of this century) the second leading cause of death among persons between 10 and 24. Suicide is more than 2 1/2 times more common than deaths from cancer in this age group. That statistic should outrage the leaders of our culture. Yet, the pace of cultural change that ultimately fuels the despair that leads to suicide quickens by the day.
While we as Christians don’t have all the answers for preventing suicide, I can’t help but believe that kids and adults who are vulnerable to mental illnesses that contribute to suicide are far better off in a church where they’re seeking to live in accordance with Jesus’ teaching than not. Our faith teaches us of the true meaning of success, provides guidance for dealing with the inevitability of adversity, instructs us as to the source of our true value and offers us protection from destructive patterns of behavior. In a broken world filled with broken brains, too many people will continue to die by their own hands. But the medical research clearly supports the idea here, here and here that faith plays an important protective role against suicidal behavior.
 Editor’s note: Here’s a link to an interview featuring Dr. Grcevich on Brian and Kathleen Mornings from Moody Radio in Cleveland in which he discusses further the findings from this study, along with ideas expressed in this post.
Editor’s note: Here’s a link to an interview featuring Dr. Grcevich on Brian and Kathleen Mornings from Moody Radio in Cleveland in which he discusses further the findings from this study, along with ideas expressed in this post.
Join Dr. G LIVE at Key Ministry’s Facebook page at 12:00 PM Eastern time on Thursday, May 5. He’ll be taking your questions for Children’s Mental Health Awareness Day. Post your questions here in advance under the comments section!
***********************************************************************************************************
 Key Ministry encourages our readers to check out the resources we’ve developed to help pastors, church leaders, volunteers and families to better understand the nature of trauma in children and teens, Jolene Philo’s series on PTSD in children, and series on other mental health-related topics, including series on the impact of ADHD, anxiety and Asperger’s Disorder on spiritual development in kids, depression in children and teens, pediatric bipolar disorder, and ten strategies for promoting mental health inclusion at church.
Key Ministry encourages our readers to check out the resources we’ve developed to help pastors, church leaders, volunteers and families to better understand the nature of trauma in children and teens, Jolene Philo’s series on PTSD in children, and series on other mental health-related topics, including series on the impact of ADHD, anxiety and Asperger’s Disorder on spiritual development in kids, depression in children and teens, pediatric bipolar disorder, and ten strategies for promoting mental health inclusion at church.

 Finding affordable care of high quality. In Northeast Ohio, we have a three-tiered healthcare system. Kids who qualify for Medicaid can access services through our teaching hospitals and community mental health centers. In some counties the available services for kids are outstanding and far exceed anything families with private insurance can access. In other counties, services are available, but child psychiatry access is limited to very brief appointments focused entirely upon prescribing of medication and counseling provided by inexperienced trainees. Sadly, the trend in our public mental health system is headed in the wrong direction. Within the last year,
Finding affordable care of high quality. In Northeast Ohio, we have a three-tiered healthcare system. Kids who qualify for Medicaid can access services through our teaching hospitals and community mental health centers. In some counties the available services for kids are outstanding and far exceed anything families with private insurance can access. In other counties, services are available, but child psychiatry access is limited to very brief appointments focused entirely upon prescribing of medication and counseling provided by inexperienced trainees. Sadly, the trend in our public mental health system is headed in the wrong direction. Within the last year,  Middle class families who depend upon their health insurance benefits may be in the most difficult situation of all. From a psychiatry perspective, the only way a physician can earn a salary comparable with those offered by public agencies while accepting insurance is to run an “assembly-line” practice composed of seeing high volumes of patients for very brief appointments. The large teaching hospitals in our area who contract with the big insurance companies won’t hire an adequate supply of clinicians to see kids with mental health issues because it’s impossible for those clinicians to see enough kids to generate the revenue necessary to cover the costs of their salaries, benefits and overhead on the reimbursement rates they get from insurance. Parents frequently get names of clinicians who are allegedly “in-network” from insurance company websites only to find that they’re not taking new patients, they don’t see kids, their offices are closed, they don’t accept the insurance in question, or that they’re scheduling six months in advance. Appointment times may not be available outside of work or school hours.
Middle class families who depend upon their health insurance benefits may be in the most difficult situation of all. From a psychiatry perspective, the only way a physician can earn a salary comparable with those offered by public agencies while accepting insurance is to run an “assembly-line” practice composed of seeing high volumes of patients for very brief appointments. The large teaching hospitals in our area who contract with the big insurance companies won’t hire an adequate supply of clinicians to see kids with mental health issues because it’s impossible for those clinicians to see enough kids to generate the revenue necessary to cover the costs of their salaries, benefits and overhead on the reimbursement rates they get from insurance. Parents frequently get names of clinicians who are allegedly “in-network” from insurance company websites only to find that they’re not taking new patients, they don’t see kids, their offices are closed, they don’t accept the insurance in question, or that they’re scheduling six months in advance. Appointment times may not be available outside of work or school hours. Editor’s note…AACAP developed
Editor’s note…AACAP developed 
 As a person struggling with mental illness reads Bible passages or hears sermons about being joyful, my encouragement is to take those commands as relating to a basic disposition of the soul toward God. Perhaps, it might be helpful to replace joy with such theological synonyms as satisfaction or rest or security or peace or acceptance. Do you have joy in the Lord? Do you believe God is on your side? Do you look to him for comfort? Are you turned toward him or away from him? Are you resting in his embrace? I think that even in the midst of depression Christians might answer yes to those questions.
As a person struggling with mental illness reads Bible passages or hears sermons about being joyful, my encouragement is to take those commands as relating to a basic disposition of the soul toward God. Perhaps, it might be helpful to replace joy with such theological synonyms as satisfaction or rest or security or peace or acceptance. Do you have joy in the Lord? Do you believe God is on your side? Do you look to him for comfort? Are you turned toward him or away from him? Are you resting in his embrace? I think that even in the midst of depression Christians might answer yes to those questions. For Gillian Marchenko, “dealing with depression” means learning to accept and treat it as a physical illness. In
For Gillian Marchenko, “dealing with depression” means learning to accept and treat it as a physical illness. In  Editor’s note: Shannon’s post was inspired by a talk she heard from Jen Hatmaker this past weekend.
Editor’s note: Shannon’s post was inspired by a talk she heard from Jen Hatmaker this past weekend. When we talk about us and them, as we often do with people with disabilities, we’re drawing lines. We wouldn’t explicitly say “we’re more human than they are,” but sometimes we say that in how we treat our friends with special needs. We say it whenever we repeat the myth that kids with Down syndrome and other conditions are sweet angels who are just happy all the time. If humans experience a range of emotions, so when we pretend like some people can’t, then we’re calling them less than human. Treating others in a condescending matter doesn’t show love.
When we talk about us and them, as we often do with people with disabilities, we’re drawing lines. We wouldn’t explicitly say “we’re more human than they are,” but sometimes we say that in how we treat our friends with special needs. We say it whenever we repeat the myth that kids with Down syndrome and other conditions are sweet angels who are just happy all the time. If humans experience a range of emotions, so when we pretend like some people can’t, then we’re calling them less than human. Treating others in a condescending matter doesn’t show love. Why risk being treated as unloveable again after the first time it’s happened? In my daughter’s dance class, another little girl refused to hold her fisted hand. Cerebral palsy made my child’s hand muscles tighten, but rejection was what made my eyes watery. This moment hasn’t been the first time and won’t be the last. Sometimes it’s easier to not even chance the rejection.
Why risk being treated as unloveable again after the first time it’s happened? In my daughter’s dance class, another little girl refused to hold her fisted hand. Cerebral palsy made my child’s hand muscles tighten, but rejection was what made my eyes watery. This moment hasn’t been the first time and won’t be the last. Sometimes it’s easier to not even chance the rejection. Check out Shannon Dingle’s blog series on adoption, disability and the church. In the series, Shannon looked at the four different kinds of special needs in adoptive and foster families and shared five ways churches can love their adoptive and foster families. Shannon’s series is a must-read for any church considering adoption or foster care initiatives.
Check out Shannon Dingle’s blog series on adoption, disability and the church. In the series, Shannon looked at the four different kinds of special needs in adoptive and foster families and shared five ways churches can love their adoptive and foster families. Shannon’s series is a must-read for any church considering adoption or foster care initiatives.  Our new ministry division for families will seek to provide encouragement and support for families of kids with disabilities through several types of online gatherings; large group communities (housed on Facebook and organized around a specific condition, disability or area of interest), special interest study groups organized around a topical study (Bible study, book study or shared media, housed on Facebook but including opportunities for real time interaction via videoconferencing) and more intimate small groups.
Our new ministry division for families will seek to provide encouragement and support for families of kids with disabilities through several types of online gatherings; large group communities (housed on Facebook and organized around a specific condition, disability or area of interest), special interest study groups organized around a topical study (Bible study, book study or shared media, housed on Facebook but including opportunities for real time interaction via videoconferencing) and more intimate small groups. Our Facebook communities will be:
Our Facebook communities will be: Special interest study groups are:
Special interest study groups are:
 Rates of mental illness are a reflection of the struggle kids and families face in responding to the external demands placed upon them by our culture. I have a very hard time with the concept of first graders carrying planners. One of the biggest changes I’ve seen in my 30 years as a doc is the increase in the productivity expectations schools place upon kids. My youngest daughter had about the same volume of homework in the first grade that I had in the seventh grade in what was then an elite public school system in Ohio. Most kids that I see with ADHD come to my office because of problems with organizational skills and work completion. Kids getting diagnosed with the condition have genuine difficulty keeping up in school. The biggest change I’ve seen in the composition of my practice involves the number of kids struggling with anxiety. The pressures to succeed both academically and socially are unprecedented.
Rates of mental illness are a reflection of the struggle kids and families face in responding to the external demands placed upon them by our culture. I have a very hard time with the concept of first graders carrying planners. One of the biggest changes I’ve seen in my 30 years as a doc is the increase in the productivity expectations schools place upon kids. My youngest daughter had about the same volume of homework in the first grade that I had in the seventh grade in what was then an elite public school system in Ohio. Most kids that I see with ADHD come to my office because of problems with organizational skills and work completion. Kids getting diagnosed with the condition have genuine difficulty keeping up in school. The biggest change I’ve seen in the composition of my practice involves the number of kids struggling with anxiety. The pressures to succeed both academically and socially are unprecedented. This comes into play when kids fail to appreciate the intensity of emotions they’ll experience when sexual boundaries are crossed. Many don’t yet have the necessary emotional maturity to manage the intensity of feelings when relationships become sexual. Kids who think too much or have a difficult time letting things go often become depressed or exhibit self-injurious behavior in response to the ups and downs of relationships. The breakdown of standards of absolute right and wrong has resulted in kids (and parents) exposed to problems and situations that they’re not equipped to deal with…a situation that frequently precipitates symptoms of mental illness in teens who are vulnerable.
This comes into play when kids fail to appreciate the intensity of emotions they’ll experience when sexual boundaries are crossed. Many don’t yet have the necessary emotional maturity to manage the intensity of feelings when relationships become sexual. Kids who think too much or have a difficult time letting things go often become depressed or exhibit self-injurious behavior in response to the ups and downs of relationships. The breakdown of standards of absolute right and wrong has resulted in kids (and parents) exposed to problems and situations that they’re not equipped to deal with…a situation that frequently precipitates symptoms of mental illness in teens who are vulnerable. One thing I struggle with most regarding my major depressive disorder is the notion that my life is a waste. There are weeks, sometimes months in the past lost to me. I look back and can’t remember what my children were like at certain ages or if we had a good time on our 2008 vacation.
One thing I struggle with most regarding my major depressive disorder is the notion that my life is a waste. There are weeks, sometimes months in the past lost to me. I look back and can’t remember what my children were like at certain ages or if we had a good time on our 2008 vacation. But even within collected black moments in life, God keeps bringing me to the Psalms of David. His hymns ease my wreaked mind and provide a moment of peace while I consider his role in the overarching theme of God’s plan of redemption. Here is a man with a tortured life, both outwardly as he is chased ruthlessly by his nemesis Saul and inwardly with the lure of another man’s wife is too much for his sinful heart to ignore. If you read David’s lyrics recorded in the Bible, you see a man familiar with darkness and yet pleading for the light, and grabbing and holding on to the moments they exist.
But even within collected black moments in life, God keeps bringing me to the Psalms of David. His hymns ease my wreaked mind and provide a moment of peace while I consider his role in the overarching theme of God’s plan of redemption. Here is a man with a tortured life, both outwardly as he is chased ruthlessly by his nemesis Saul and inwardly with the lure of another man’s wife is too much for his sinful heart to ignore. If you read David’s lyrics recorded in the Bible, you see a man familiar with darkness and yet pleading for the light, and grabbing and holding on to the moments they exist. We’re going to plunge headfirst into a topic this week that I’ve never seen addressed anywhere in books, articles or seminars on working with families of kids with ADHD…the use of medication for the specific purpose of helping kids function better during church-based programs and activities.
We’re going to plunge headfirst into a topic this week that I’ve never seen addressed anywhere in books, articles or seminars on working with families of kids with ADHD…the use of medication for the specific purpose of helping kids function better during church-based programs and activities.

 Scheduling of activities for children and youth can create challenges for medication administration. There’s a big pool of kids out there for whom their needs for support in church will vary from activity to activity. The parent who gives their kid his medicine two hours before leaving for church may not send medication along for a weekend retreat. If your church offers AWANA (or similar midweek programming) and has a high percentage of kids with ADHD, it’s important to keep in mind that the three most commonly prescribed medications for ADHD (Adderall XR, Concerta and Vyvanse) typically wear off around dinnertime when kids take medication before leaving for school.
Scheduling of activities for children and youth can create challenges for medication administration. There’s a big pool of kids out there for whom their needs for support in church will vary from activity to activity. The parent who gives their kid his medicine two hours before leaving for church may not send medication along for a weekend retreat. If your church offers AWANA (or similar midweek programming) and has a high percentage of kids with ADHD, it’s important to keep in mind that the three most commonly prescribed medications for ADHD (Adderall XR, Concerta and Vyvanse) typically wear off around dinnertime when kids take medication before leaving for school. The other side to this discussion involves the perspective of the child’s prescribing physician/clinician. Why wouldn’t the kid’s doctor instruct parents to use medication on Sundays or for evening church activities?
The other side to this discussion involves the perspective of the child’s prescribing physician/clinician. Why wouldn’t the kid’s doctor instruct parents to use medication on Sundays or for evening church activities? Editor’s Note: Ryan Wolfe and Shannon Dingle are in suburban Washington D.C. this weekend presenting at the McLean Bible Church Accessibility Summit. Ryan’s had a busy week…we’re sharing a post from
Editor’s Note: Ryan Wolfe and Shannon Dingle are in suburban Washington D.C. this weekend presenting at the McLean Bible Church Accessibility Summit. Ryan’s had a busy week…we’re sharing a post from 

 Gillian Marchenko’s new book,
Gillian Marchenko’s new book, 




