Here’s the second segment in our series for Mental Health Month… Ten things I wish church leaders knew about families and mental illness. Today, we’ll share some information about the prevalence of mental illness in children and adults, and look at why the numbers should move church leaders to respond.
Here’s the second segment in our series for Mental Health Month… Ten things I wish church leaders knew about families and mental illness. Today, we’ll share some information about the prevalence of mental illness in children and adults, and look at why the numbers should move church leaders to respond.
In a candid moment, most church leaders are willing to express that they monitor church attendance figures and that the numbers of people attending church are a significant ongoing concern among pastors and church staff. Nationwide, statistics examining church attendance likely overreport the numbers of Americans who come to church. Several recent estimates suggest only 18-25% of the U.S. population regularly attend a Christian church on weekends. Lower attendance may suggest that fewer people are being impacted by a church’s ministry activities and suggests less money and volunteers will be available to support the church’s mission. Outreach to the community and inclusion of new attendees are generally high on the list of priorities of the typical pastor or church board.
Families impacted by disability, especially families impacted by mental illness, trauma and developmental disabilities, would in my mind represent a largely underserved population for local churches for the following reasons…
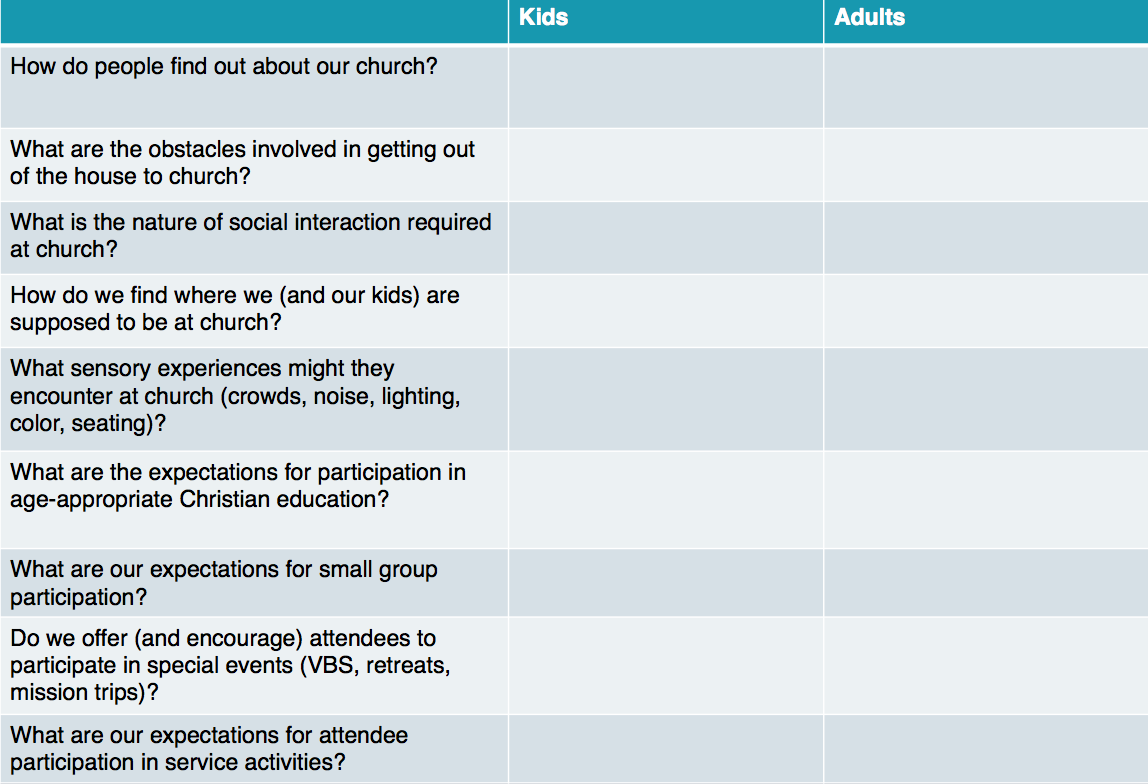
- There are lots of individuals and families impacted by common mental health conditions living in close proximity to local churches who don’t currently attend church, in part because their conditions present subtle, but real barriers to church involvement, as we discussed here last week.
- Most children and adults with mental illness can be successfully assimilated at church without the need to create new programs or ministries.
- In addition to the value of the Gospel, churches can offer opportunities for relationship and practical supports that many families impacted by mental health concerns would find helpful.
Let’s focus today on the size of the “mission field next door” and look at some statistics from the National Institute of Mental Health about common conditions that present barriers to church attendance…
Here are some statistics on anxiety prevalence and treatment in adults…I’d suggest that it is highly unlikely that an adult with severe anxiety is regularly attending church, and significantly less likely that adults who meet criteria for an anxiety disorder attend regularly. Of note…the peak in anxiety prevalence occurs in 30-44 year old women…the very people we depend on to bring children to church!


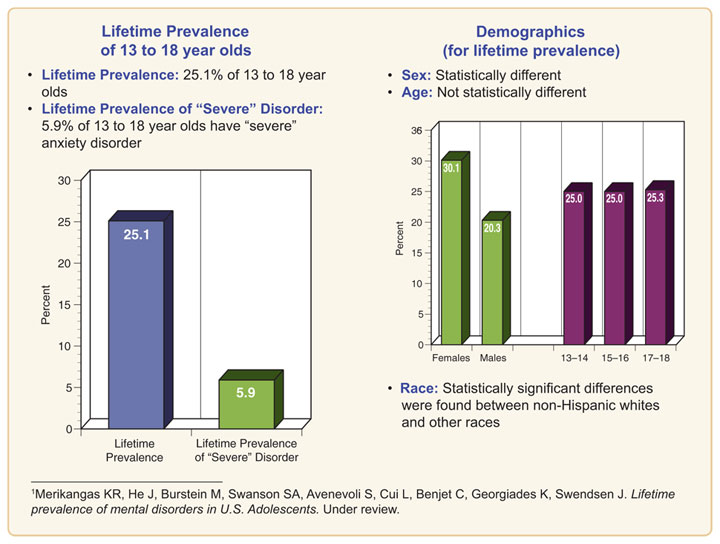
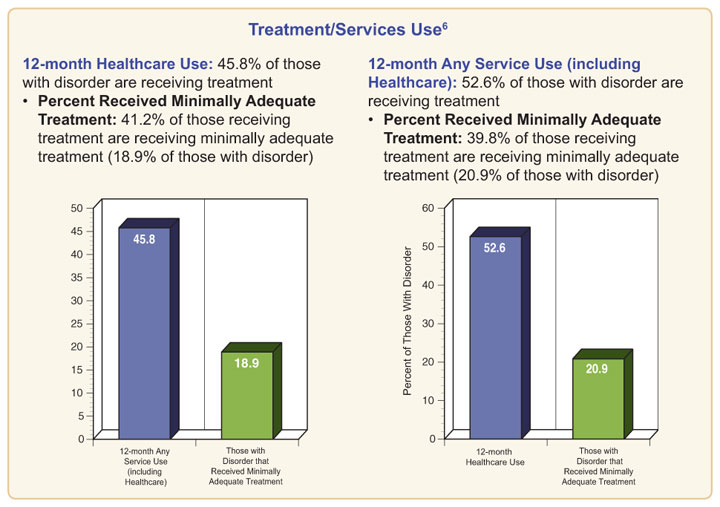
Here are the statistics looking at anxiety prevalence in teens…we’re almost certainly missing most of the 5.9% of teens with “severe” anxiety and a significant chunk of the one in four teens who have experienced an anxiety disorder in their lifetimes…
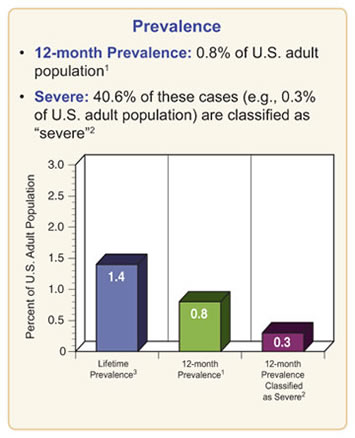
Let’s look at agoraphobia specifically, because attending a weekend worship service in a reasonably crowded church is probably the most challenging activity for the kids in our practice we treat with the condition. Again…if the child or adult with agoraphobia can’t attend church, there’s a very good possibility that no one in the family is attending church!
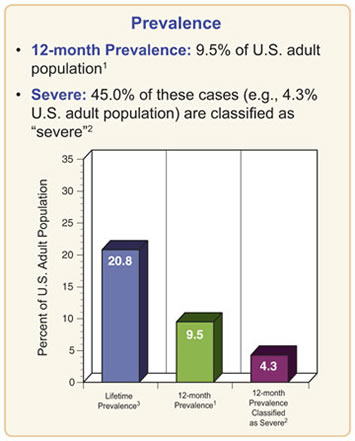
Now…let’s look at mood disorders in adults…keeping in mind that roughly 50% receive treatment, 45% are classified as “severe” and that only 38.5% receive “minimally adequate treatment.” These conditions are likely to impede church attendance during periods when symptoms are more severe…

And mood disorders in teens…

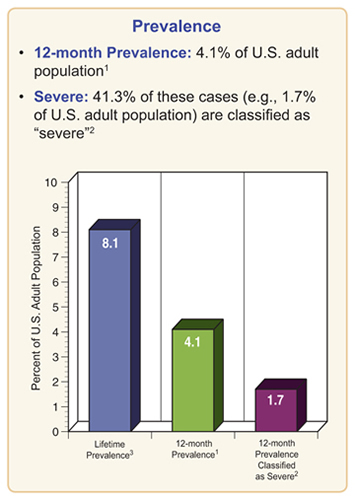
Finally, let’s look at ADHD in adults. They’re likely to have more difficulty making church a priority, getting up on time, and organizing themselves (and their children) to get to church on time…
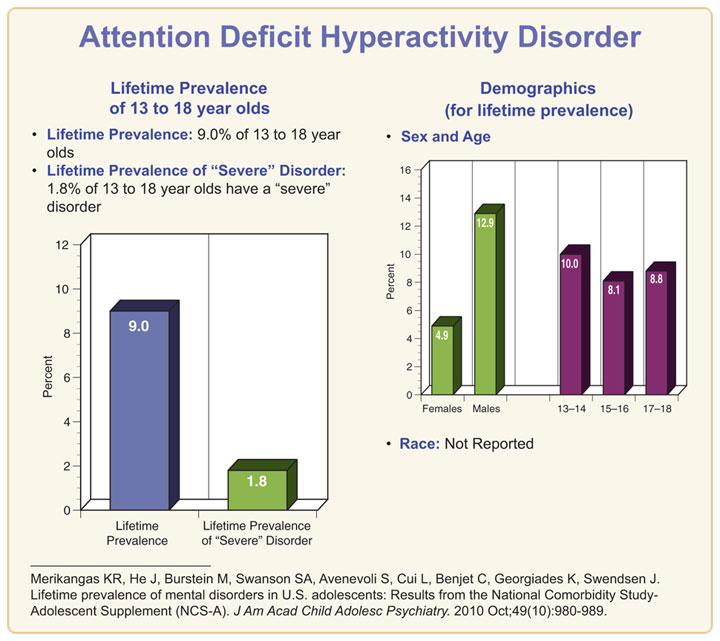
And ADHD in kids…those who struggle with impulse control and emotional self-regulation will experience significant difficulty in the typical children’s ministry environment or large group worship services, while teens with ADHD will experience challenges similar to adults with ADHD…
So church…we have literally hundreds of kids and hundreds of families living in close proximity to our churches with conditions that pose barriers to church attendance that can be addressed with some intentionality at relatively little cost without an excessive drain on staffing or volunteer resources! What are we waiting for?
Updated January 12, 2018
***********************************************************************************************************
 Key Ministry has assembled resources to help churches more effectively minister to children and adults with ADHD, anxiety disorders, Asperger’s Disorder, Bipolar Disorder, depression and trauma. Please share our resources with any pastors, church staff, volunteers or families looking to learn more about the influence these conditions can exert upon spiritual development in kids, and what churches can do to help!
Key Ministry has assembled resources to help churches more effectively minister to children and adults with ADHD, anxiety disorders, Asperger’s Disorder, Bipolar Disorder, depression and trauma. Please share our resources with any pastors, church staff, volunteers or families looking to learn more about the influence these conditions can exert upon spiritual development in kids, and what churches can do to help!