Although letting go of control is awful, pretending to be in control of that which we are not is even worse. Besides, it is only through the holes in the fence that beauty enters in, along with the pain. Our structures of protection serve to keep out blessing as well. All is intertwined and wound up together , pain and beauty, and both advance only as the fences fall and the gate swings open.
Although letting go of control is awful, pretending to be in control of that which we are not is even worse. Besides, it is only through the holes in the fence that beauty enters in, along with the pain. Our structures of protection serve to keep out blessing as well. All is intertwined and wound up together , pain and beauty, and both advance only as the fences fall and the gate swings open.
I thought A Story Unfinished was going to be about disability-the story of how God was at work through Matt and Ginny Mooney’s experience as parents of a boy (Eliot) who lived for 99 days with a genetic disease (Trisomy 18) that had made his birth unlikely. After all, Matt is a visionary leader within the disability ministry movement currently serving as Executive Director of 99 Balloons, a non-profit organization based in Northwest Arkansas that helps others engage children with special needs locally and globally. But the book isn’t really about disability…instead, A Story Unfinished is a testimony from a remarkably faithful young Christian couple that touches upon much broader issues that produce tension and conflict for people of all ages who seek to better understand the ways of Jesus.
Matt’s authenticity in describing his attempts to maintain a sense of control over life’s circumstances while avoiding pain at all costs is a mindset I identify with-and a very common mindset among my friends and neighbors. We desire to be safe…especially those of us who are part of the church. Our local contemporary Christian radio station markets itself as “safe for the whole family.” An unspoken desire of many church families with school-age children is that a faith-based upbringing will protect their kids from the emotional, physical and legal consequences of choices that run counter to the teachings of Scripture. Matt points out the impossibility of truly following Christ while avoiding pain.
Only by faith, and never by reason, do we stand in line for the very ride that all within us says to avoid. Jesus plunged headfirst into the swirl of the Cross-the one He prayed to avoid if at all possible. Scripture informs us that the lifeless body of Christ was laid in a tomb, where it remained for three days until He arose, overcoming death and ascending to heaven to reside with the Father on the day we commemorate as Easter Sunday. In my former bifurcated life, Easter is good, but Friday is not.
Matt’s book is really about submission…giving up our agendas and sense of self-sufficiency for a life in which we experience both pain and joy in the process of truly experiencing the presence of God through becoming totally dependent upon Him.
The Cross reminds us that God’s hope for us does not lie in temporary, status-quo safety. Instead, He asks us to trade in our most intimate desires for a life of faith-the kind of faith that does not allow for constructing safety nets, the kind of faith through which He is enough, and He is all we have.
I hope A Story Unfinished receives exposure far beyond the disability ministry community. It was the most challenging book I’ve read on Christian living in several years, cutting to the core of issues with which we all struggle far more than we’re willing to admit.
***********************************************************************************************************
 At thirty weeks pregnant Matt Mooney and his wife Ginny were informed that their child had a genetic disease Trisomy 18.
At thirty weeks pregnant Matt Mooney and his wife Ginny were informed that their child had a genetic disease Trisomy 18.
They were told that birth was unlikely.
That life was not viable.
That a bleak future awaited.
They were not told that they would get 99 days with this child and these precious days would change them forever. Through the sleepless nights, an unrelenting desire for answers, and the frightening reality that slides in where optimism once resided, Matt and Ginny walked with family and friends through the life and death of their first born son.
At Eliot’s funeral, 99 balloons were released into the air to represent the 99 days of his life. This act of remembrance stirred the hearts of a community and a country.
The story of Eliot was featured on Oprah and the Today show. A video of his life was watched by millions on Youtube. But the story of Eliot’s life and death is not the end of this journey. Through the impact of his life, a legacy has continued.
A Story Unfinished chronicles a father’s journey of pain and redemption and the mystery of God and His goodness in the midst of it all.
Available at Amazon and booksellers everywhere.







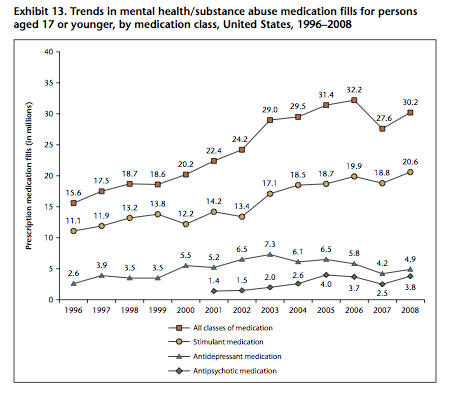







 Our current blog series… Dissecting the DSM-5…What it Means for Kids and Families, continues today with an examination of the recently updated diagnostic criteria for Oppositional Defiant Disorder.
Our current blog series… Dissecting the DSM-5…What it Means for Kids and Families, continues today with an examination of the recently updated diagnostic criteria for Oppositional Defiant Disorder. Other kids are disrespectful and struggle with transitions because of their inability to let go of their mental script of how a given interaction or situation should unfold. They correspond to the argumentative/defiant group in ODD. They perseverate or get “stuck” on a picture in their mind of how things should be and escalate when adults violate their sense of control. The first subset of kids is defiant because they can’t stop and think. The second subset is defiant because they can’t tolerate the inner frustration when events unfold differently than they’ve pictured in their minds. We know kids who “ruminate” or perseverate often experience problems with anxiety and/or depression as they get older.
Other kids are disrespectful and struggle with transitions because of their inability to let go of their mental script of how a given interaction or situation should unfold. They correspond to the argumentative/defiant group in ODD. They perseverate or get “stuck” on a picture in their mind of how things should be and escalate when adults violate their sense of control. The first subset of kids is defiant because they can’t stop and think. The second subset is defiant because they can’t tolerate the inner frustration when events unfold differently than they’ve pictured in their minds. We know kids who “ruminate” or perseverate often experience problems with anxiety and/or depression as they get older.