For the first time in several years I had the opportunity to attend the American Academy of Child and Adolescent Psychiatry’s Annual Meeting, held this year in one of my favorite cities…Orlando, Florida.
In a later series of posts, I’ll share a little more about the overall tone of the meeting and my sense of where the field of children’s mental health is headed. Tonight, I thought I’d share some brief summaries of several studies I found interesting…
Dr. Elizabeth Brownlie and her colleagues from the University of Toronto have observed that youth with language impairment have high rates of anxiety and social problems and may be vulnerable to social anxiety in adulthood. They compared a cohort of children with language impairment and typical language controls in rates of social phobia and subclinical social anxiety symptoms from age 5 to ages 19, 25 and 31 in a prospective longitudinal study (n = 142) at age 5 to matched control group (n = 142). Childhood language impairment was found to be associated with subclinical levels of social anxiety in early adulthood, particularly related to social interaction. The findings support the notion that communication difficulties in childhood may lead to social anxiety in adults.
One of the challenges we face as clinicians when treating kids with depression is accurately describing to parents the additional benefits of combining cognitive-behavioral therapy (CBT) with medication. A study by Dr. Manesh Aligeti and colleagues at UT Southwestern Medical School looked at the benefits of CBT for relapse prevention in a sample of 8-17 year-old patients (N=144) who had been positive responders to fluoxetine. The only impact the CBT appeared to have on medication management involved the use of lower doses of fluoxetine among the kids who were also receiving therapy. Examining the same patient sample, Dr. Graham Emslie found that kids receiving CBT in addition to medication had a significantly lower risk of relapse than those receiving medication alone during the 30-week continuation treatment period of the study. The estimated probability of relapse was 7.5% among kids receiving medication and CBT vs. 28% among kids receiving CBT alone.
Dr. Linmarie Sikich and her team at the University of North Carolina sought to determine the tolerability and efficacy of extended treatment with intranasal oxytocin (a pituitary hormone referred to by some as the “bonding hormone”) as a supplemental treatment for children and adolescents with an autism spectrum disorder. Measures of social reciprocity and social functioning showed improvement in the oxytocin group vs the placebo group. The improvements persisted and were more noticable with extended (16 week) treatment. There was no difference in adverse effects of the treatment group versus children and teens who received placebo. Oxytocin appears to have been well tolerated by most children over 16 weeks of sustained treatment. The hormone appeared to reduce irritability and improve some aspects of social functioning in a sample of 3-17 year-old patients with autism spectrum disorders.
Finally, in an issue that hits close to home and has been a long-term concern of mine, a team from The Ohio State University compared polypharmacy patterns and rates over time among kids in foster care (FC), kids with disabilities (ABD), and low income kids (CFC) who qualified for Medicaid. Kids ages 17 years and younger who were continuously enrolled in Ohio Medicaid for a 1-year period and prescribed at least one psychotropic medication (antidepressants, antipsychotics mood stabilizers, stimulants, alpha-agonists and anxiolytics) during fiscal years 2002 (n = 26,252) through 2008 (n = 50,319) were selected. Polypharmacy was defined as ≥ 3 medications and multi-class polypharmacy as ≥ 3 medications from different drug classes. Both types of polypharmacy increased across all three eligibility groups. Polypharmacy increased from 8.8% to 11.5% for CFC youth, from 18.0% to 24.9% for ABD youth and from 19.8% to 27.3% for FC youth. Combinations that increased the most were two or more antipsychotics, two or more stimulants, and antipsychotics with stimulants and other psychotropic medications excluding antidepressants. Highest rates of polypharmacy were noted among youth in foster care.
AACAP Resource Centers empower consumers through patient education. Each AACAP Resource Center contains consumer-friendly definitions, answers to frequently asked questions, clinical resources, expert videos, and abstracts from the JAACAP, Scientific Proceedings and Facts for Families relevant to each disorder. Check out AACAP Resource Centers on ADHD, anxiety disorders, autism, bipolar disorder, bullying, child abuse, Conduct Disorder, depression, disaster, military families, Oppositional Defiant Disorder and substance use by clicking here.
As we near next week’s conclusion of our blog series on trauma in children and teens, Jolene Philo’s presentation from last year’s Inclusion Fusion on PTSD and kids with special needs seemed like the perfect compliment.
Jolene is the author of two books for parents of children with special needs, A Different Dream for My Child and Different Dream Parenting. She is the parent of a child with special needs who developed PTSD due to early, frequent and invasive medical treatment. She also taught traumatized students at a correctional facility and collaborated with special education teachers to mainstream traumatized children in her classroom during public school teaching career. She’s conducted extensive interviews with trauma experts and is currently working on a book about PTSD in children. More information about PTSD and kids can be found at her website, A Different Dream.
Jolene and our former colleague Katie Wetherbee signed a contract for a book titled Every Child Welcome: A Menu of Strategies for Including Kids with Special Needs at Church. Every Child Welcome is geared for volunteers who work with children’s ministry. It will be jam-packed with practical and doable inclusion strategies children’s ministry volunteers can implement so every child feels welcome.
Post-Traumatic Stress Disorder (PTSD) is a mental disorder most commonly associated with combat veterans that also affects children with special needs. In Jolene’s presentation, she discusses six common myths and misconceptions about PTSD in children.
Our Key Ministry website is a resource through which church staff, volunteers, family members and caregivers can register for upcoming training events, request access to our library of downloadable ministry resources, contact our staff with training or consultation requests, access the content of our official ministry blog, or contribute their time, talent and treasure to the expansion of God’s Kingdom through the work of Key Ministry. In addition to our downloadable resources, those who register for our resource kit can view any presentation from our Inclusion Fusion Disability Ministry Web Summits “on-demand”. All of these resources are made available free of charge. Check out our website today!
Welcome to the ninth installment of our Fall 2013 blog series: Trauma and Kids…A Primer for Pastors, Church Staff and Parents. Today, we’ll look at therapeutic approaches to treating children and teens following a traumatic event(s).
Today, we’re going to take a closer look at evidence-based strategies for treating children and teens following a traumatic event.
Before we begin today, I’ll note that there’s not a great deal of evidence suggesting that the early response teams are especially helpful in preventing PTSD among children and teens following disasters or school shootings.
The treatment approach with the most support in the research literature is trauma-focused cognitive-behavioral therapy (TF-CBT). TF-CBT has been demonstrated superior to other non-specific or non-directive therapies in kids from preschool age through adolescence. The critical component of the treatment involves directly addressing the child or teen’s traumatic experiences in therapy. Kids aren’t inclined to focus on their trauma when given a choice of topics to address during therapy visits. The timing and pacing of the therapy are based upon the child’s responses as monitored by the parent and the therapist. Other critical components of the treatment include including the child’s parents as agents of change, and a focus on prevention of future trauma, along with the development of resiliency.
An acronym summarizing the key components of TF-CBT is PRACTICE…
Psychoeducation… Teaching kids and parents about the type of traumatic event the child experienced, common reactions to trauma, along with Parenting skills… Praise, positive attention, selective attention, contingency reinforcement
Relaxation skills…
Affective modulation…feelings identification, positive self-talk, problem-solving, thought interruption, positive imagery
Cognitive coping and processing…recognizing connections between thoughts, feelings and behaviors, addressing “thinking errors” and misperceptions
Trauma narrative…developing a narrative of the child/teen’s experiences, correcting cognitive distortions and placing the traumatic event(s) in the context of the child’s life.
In-vivo exposure…graduated exposure to fear-inducing stimuli
Conjoint child-parent sessions…the child/teen shares their trauma narrative with parents/family, family issues are addressed.
Enhancement of future safety…prevention of future trauma and return to a typical developmental trajectory
Another “manualized” form of TF-CBT is CBITS (Cognitive-Behavioral Intervention for Trauma in Schools). CBITS includes all of the components of the PRACTICE model except for the parent component of treatment, but does include a teacher component addressing the possible impact of trauma upon learning.
Seeking Safety is a specific TF-CBT protocol used for teens with PTSD and comorbid substance use issues. There is less evidence to support psychodynamic psychotherapy as a treatment intervention for trauma and teens.
EMDR (Eye Movement Desensitization and Reprocessing) has been demonstrated to be an effective treatment intervention for ADULTS with PTSD. There is one randomized trial of children with PTSD in Sweden showing benefit from EMDR, using a protocol with significant deviations from approaches used in adults, both in interventions and techniques.
Next: What do we know about the use of medication in kids with PTSD?
Our Key Ministry website is a resource through which church staff, volunteers, family members and caregivers can register for upcoming training events, request access to our library of downloadable ministry resources, contact our staff with training or consultation requests, access the content of our official ministry blog, or contribute their time, talent and treasure to the expansion of God’s Kingdom through the work of Key Ministry. In addition to our downloadable resources, those who register for our resource kit can view any presentation from our Inclusion Fusion Disability Ministry Web Summits “on-demand”. All of these resources are made available free of charge. Check out our website today!
Welcome to the eighth installment of our Fall 2013 blog series: Trauma and Kids…A Primer for Pastors, Church Staff and Parents. Today, we’ll look at some of the challenges clinicians face in separating the effects of trauma from the signs and symptoms of mental illness in children and teens.
One of the challenges we face in treating kids with trauma is sorting out the extent to which the symptoms leading to referral are trauma-related, or associated with some other mental health disorder in which the symptoms are totally unrelated to the trauma.
Kids with trauma histories frequently present with marked dysregulation of affect, mood and behavior…not surprising, when one considers the impact of trauma on brain development discussed earlier in this series. Children of parents with chronic mental illness are more likely to live in the types of chronically dysfunctional environments in which traumatic events are more likely to occur.
Some of the conditions that can mimic symptoms associated with trauma/PTSD include…
ADHD: Kids will often present with agitation, restlessness, decreased concentration, hyperactivity, hyperarousal and difficulty with sleep.
Oppositional Defiant Disorder: Some kids may manifest PTSD primarily through angry outbursts and/or irritability.
Panic Disorder: Kids and teens can manifest symptoms that mimic panic attacks when they encounter reminders that trigger distressing memories of traumatic events.
Social Anxiety Disorder: avoidance and social withdrawal are common coping mechanisms among children and teens who have experienced trauma.
Depression: Affective numbing associated with trauma, in conjunction with sleep disturbances, avoidance of people, self-injurious behavior can frequently be misdiagnosed as depression.
Bipolar Disorder/Disruptive Mood Dysregulation Disorder: Irritability and mood lability in in kids following traumatic events, in addition to hypersexualized behavior in kids exposed to sexual trauma may lead to a misdiagnosis of a mood disorder.
There was some discussion around the development of the DSM-5 regarding a condition referred to as chronic PTSD in kids and teens with exposure to early, severe or interpersonal trauma…or complex PTSD…a condition occurring in conjunction with other DSM conditions.
I find it helpful when kids appear to manifest symptoms of other psychiatric disorders following a traumatic event(s) to ascertain whether the. symptoms of other mental health disorders preceded the trauma. When possible, we would seek to treat the comorbid conditions in an integrated manner that helps “kill two birds with one stone.” I’ll address treatment specifically in our next two posts.
Confused about all the changes in diagnostic terminology for kids with mental heath disorders? Key Ministry has a resource page summarizing our recent blog series examining the impact of the DSM-5 on kids with mental health disorders. Click this link for summary articles describing the changes in diagnostic criteria for conditions common among children and teens, along with links to other helpful resources!
Earlier today, I had the honor and joy of worshiping with the people of St. Mark’s UMC in Findlay, OH. They’re seeking to welcome lots of kids and families to their church who aren’t currently part of the church because of the barriers presented by mental illness, trauma and developmental disabilities. I wanted to share with our readers the message I shared today at St. Mark’s…
Thanks to Michelle and the leadership team of St. Mark’s Findlay for inviting me to be with you today. I’ve had a chance to do some pretty cool stuff in the course of my career, but there’s no greater honor than to be invited to teach from God’s Word in God’s house.
I’d be willing to bet it’s not every Sunday that you come to church and find yourself listening to a message from a physician who specializes in child and adolescent psychiatry. But I don’t think my presence here this morning is an accident. Allow me to introduce myself and share how I came to be here.
I wear lots of “hats” in my work. I teach at both Case Western Reserve and Northeast Ohio Medical University, I’ve been involved in a fair amount of clinical research, and I lead a group practice in Chagrin Falls.
Around fifteen years ago, a number of well-established families from our church adopted kids with very complex emotional, behavioral and developmental issues from orphanages in Russia and Bulgaria. Our children’s ministry director at the time (a speech and language pathologist by training) spoke of the steps the staff was taking to help the families affected stay connected with church…None of the kids being served had obvious, outward signs of disability, but the severity of their behavior had become a major obstacle to their families in maintaining their involvement with the church.
I went back to my practice was quite surprised to discover that the conditions we were treating at that time appeared to present significant limitations to our families in attending worship services and maintaining an active involvement in the church. This really bothered me…my family has been blessed by the opportunity to experience what most of us here this morning can easily take for granted…the opportunity to regularly attend a church where we came to know Jesus. I want other families…the families I see every day through our practice to have the same opportunity my family had…the opportunity to grow in faith while a part of a caring and supportive church family.
Over the next few years, God opened lots of doors for me. I was involved with research that provided me the opportunity to travel widely. Wherever I went, I talked about the work our church back home was doing…and our church started getting LOTS of requests for help and support. As more and more clergy, professionals and family members recognized the need to help churches connect with families of kids with what we referred to as “hidden disabilities”, a group of us launched Key Ministry over ten years ago to provide knowledge, innovation and experience to the worldwide church as it ministers to and with families of children impacted by mental illness, trauma and developmental disabilities.
This past summer, our team was here in Northwest Ohio putting on training for churches interested in serving families of kids with disabilities. I’m here this morning because some leaders from your church who attended that training believe that God may be positioning you to minister with a large group of families here in Findlay and Hancock County who very much need to experience His love…families, without whom, we as a church are incomplete.
You’re literally sitting in the middle of an enormous mission field and you may not even know it. If you’re like me, when you think of missions, you think of some third world country. No high-speed Internet. No electricity. Digging wells. Building huts. That’s not me. I’m not good with my hands. There’s a reason I’m not a surgeon. But God has placed you in a mission field that you won’t need a passport to check out.
Who do you think of when you hear the terms “disabilities” or “special needs”?
You may think of people with physical disabilities…leaders like Joni Earickson Tada and Nick Vujicic.
When you hear the term “special needs ministry” what comes to mind? For many people, the answer would be kids with intellectual disabilities…But when we consider disability as a barrier to families becoming involved with church, our existing ministries are just beginning to scratch the surface.
Allow me to introduce you to “the mission field next door.”
Here’s the definition of “disability” from the Americans With Disabilities Act (1990)
I’d ask you-from a mental or physical impairment substantially limits a person’s ability to pursue spiritual growth and participate in a local church, might we consider that person “disabled?” I’d think so.
The obstacles that exist to a person with a physical disability attending church are pretty obvious. But let’s consider for a minute the barriers to “doing church” for someone with mental illness, trauma or a developmental disability…or the family of a child with one of those disabilities. According to the National Institute of Mental Health, mental illness is the #1 cause of disability in the U.S. There are lots of things about the environments in which we “do church” that present subtle, but very real obstacles to kids and families impacted by these disabilities in attending worship and participating in the other stuff we do to help kids and their parents grow spiritually. Let’s take a closer look at the obstacles they face…
Kids with mental illness, a history of trauma, abuse or developmental disabilities are more likely to experience…
Difficulties with self-control and self-regulation of emotion: Let’s face it…we expect kids to act a certain way when they’re at church. Some kids have to expend much more effort maintaining self-control than their peers…and the more stimulation they have to process at any given moment, the more difficult it may be for them to maintain self control. We as Christians start making assumptions about the parents when kids struggle with self-control for no obvious reason. I hear from parents all the time who have left church because they sensed they were being judged by the behavior their kids exhibited at church.
Our church had a Disability Ministry Sunday in which the parents of two young boys with ADHD were given the opportunity to share their story at each of our worship services. They told of their struggle to find a church they could attend as a family-and the reactions…mainly dirty looks…they received from others when visiting different churches. The mom shared this statement that summaries the experience of church many families share…
“”People in the church believe they can tell when a disability ends and bad parenting begins”.
Sensory processing issues: Many kids, teens and adults with autism spectrum disorders, anxiety disorders or ADHD process sensory input differently than the rest of us. They might experience physical touch, our worship music, the lighting in the children’s ministry area, or the sound of many people talking at once on the way in or way out of church as distressing.
Fear of the unknown: Research has shown that one of the core differences in brain functioning among kids and adults with anxiety disorders is their propensity to overestimate the potential risks associated with new situations. Kids (and their parents) attending a new church will frequently need to overcome unspoken (and often irrational) fears.
Shame/potential for embarrassment: Someone with panic disorder who is more vulnerable to attacks around crowds may be very uncomfortable sitting in your sanctuary/worship center on a busy Sunday morning. Or how might a kid with dyslexia feel in a Sunday school class where kids are expected to take turns reading from the Bible?
Social isolation: Families of kids with disabilities frequently lack relationships with others who might invite them to church. Their children are less likely to have friends who’ll invite them to Vacation Bible School. They’re less likely to connect with other families through sports or extracurricular activities. The divorce rate among couples of kids under the age of 8 with ADHD is twice that of the general population. The kids may be shuffled from one parent to another on alternating weekends, disrupting the continuity of any church experience. The parents may have fewer friends as a result of the financial demands and time demands of their child’s disability. They can’t use just any teen as a babysitter on Saturday night.
Lack of social skills to navigate relational demands of church: Think about a kid who gets made fun of at school as a result of being socially awkward…maybe they don’t intuitively pick up on how they’re supposed to act in a new situation. Maybe they don’t process social cues in the way other kids do. When they leave familiar friends and adults in children’s ministry for middle school ministry, or enter high school ministry where they’re expected to attend a house group in an unfamiliar place surrounded by older kids already comfortable with their friends, they may fall away from church.
Families overwhelmed by demands of daily life: The demands of getting through the week with a child with a disability may be so great that the thought of getting the kids ready for church on Sunday morning may be overwhelming. It may be easier for mom to crawl back into bed instead of facing meltdowns when she needs to tear her kid away from the Xbox to get ready for church.
You literally have families living within the shadow of your steeple struggling with these issues…Here are a few statistics:
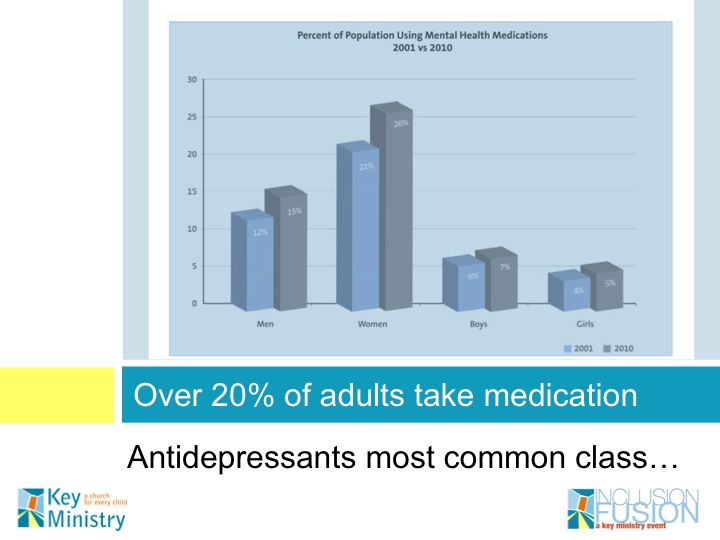
22% of U.S. children entering first grade…and 26% of adults meet criteria for at least one mental health disorder
11% of 5-17 year olds have received at least one prescription for ADHD medication
8% of teens have anxiety disorders-most have been symptomatic since age 6 (and only 18% have received treatment)
13% of kids in the U.S. are diagnosed with at least one developmental disorder
One child in 91 has an autism spectrum disorder
Let’s keep in mind that kids with disabilities often have parents with disabilities. And lest we think this is only an issue for the kids, we live in a country where more than one in five adults…and one in four women are prescribed some form of psychiatric medication. Most are on antidepressants… used more commonly for anxiety than depression…and the use of these medications increased by 28% among men and 29% among women during the past decade.
The bottom line is that kids with mental health issues, kids who have experienced trauma, kids with developmental disabilities…and adults with these conditions have a much harder time functioning in the environments in which we “do church”. They face additional obstacles in getting to Jesus…and that brings us to our Scripture today, on some friends who had a friend who needed to meet Jesus.
If you brought your Bibles please turn to the Gospel of Mark, Chapter 2, verses 1-12:
And when he returned to Capernaum after some days, it was reported that he was at home. And many were gathered together, so that there was no more room, not even at the door. And he was preaching the word to them. And they came, bringing to him a paralytic carried by four men. And when they could not get near him because of the crowd, they removed the roof above him, and when they had made an opening, they let down the bed on which the paralytic lay. And when Jesus saw their faith, he said to the paralytic, “Son, your sins are forgiven.” Now some of the scribes were sitting there, questioning in their hearts, “Why does this man speak like that? He is blaspheming! Who can forgive sins but God alone?” And immediately Jesus, perceiving in his spirit that they thus questioned within themselves, said to them, “Why do you question these things in your hearts? Which is easier, to say to the paralytic, ‘Your sins are forgiven,’ or to say, ‘Rise, take up your bed and walk’? But that you may know that the Son of Man has authority on earth to forgive sins”—he said to the paralytic— “I say to you, rise, pick up your bed, and go home.” And he rose and immediately picked up his bed and went out before them all, so that they were all amazed and glorified God, saying, “We never saw anything like this!”
Let’s dig into today’s passage a little more closely…
Jesus is in Capernaum…the text says that He’d “returned to Capernaum”…so where had He been? Mark 1:45 tells us He had been in “desolate places”. Why was He in desolate places? Look back at Mark 1:40. Jesus healed a man with leprosy and “sternly charged” him to say nothing about his healing, but to present himself to the priest. The verb for “sternly charged” in the Greek also appears in John 11:33 when Jesus is at Lazarus’ tomb, translated there as “deeply moved”. The implication is that Jesus was VERY emotional in imploring this man to lay low. When he disobeyed Jesus, Jesus became a “marked man”.
There were lots of people in need of healing back in that day. The average life expectancy in first century Palestine was around 30. Most people were below age 45. Without modern medicine…and a social safety net…disability truly represented a life crisis. And Jesus healed everybody. This was a problem…the healing ministry was becoming a huge distraction from Jesus’ teaching ministry.
This entire passage is really about Jesus attempting to reveal His true identity to the assembled people and religious authorities.
Jesus drops all kinds of hints to his identity throughout this story. Through His healing, Jesus demonstrates his power over the effects of sin in a fallen world. He’s also claiming to have the power to forgive sin. Jesus gives them another hint at His true identity by demonstrating his ability to read their hearts and minds! (See Genesis 6:5, Psalms 19:14) The religious leaders were onto something when they thought Jesus was a blasphemer… they recognized that Jesus was making claims only God could make. They (and we) are left with three possible conclusions when considering Jesus’ claims. Either Jesus is delusional or a liar or He’s telling the truth.
What I find truly amazing in this story is the lengths to which the friends were willing to go to get their disabled friend in front of Jesus, even though they didn’t really grasp who Jesus was. They had a natural faith. Jesus recognized their faith…but their faith is like the faith we have when we go to Cleveland Clinic for surgery. We place our trust in doctors and hospitals with track records of healing sick people…and Jesus had a track record. But why did Jesus only forgive the sins of the man who was paralyzed and not the sins of his friends?
There’s a difference between recognizing who Jesus is and acknowledging that we’re sinners in need of a Savior, incapable of saving ourselves. After all, in James 2:19 we’re told that demons believe…they’re unwilling to submit to God!
For our sins to be forgiven, we have to acknowledge our need for forgiveness. Maybe something about the physical brokenness experienced by the man with paralysis enabled him to acknowledge his spiritual brokenness to God? As Jesus read the hearts of the religious leaders in the room, He also saw into in the heart of the man with paralysis…and extended His forgiveness.
Unlike the friends on the roof and the audience in the room, presumably we in the church understand who Jesus is. We have the Bible and the Holy Spirit to help us understand God’s Word. We have personal experiences of what Jesus has done in our lives and the lives of those around us. So…why aren’t we doing more to introduce others to Jesus in need of forgiveness and salvation?
On to a second observation…the people in the crowd were so into their own agendas that they were oblivious to the need of the man with paralysis. We can probably assume from the story that the friends tried the door first. You’d think the crowd would make room for a stretcher with a famous healer in the middle of the room. But they were obviously thinking about other things.
In first century Galilee, people in the crowd likely assumed that the disabled man (or someone in his family) had committed a sin. Recall John 9:1, when the disciples questioned Jesus about the cause of a blind man’s condition. The Jewish people…particularly, their religious authorities, considered themselves morally and spiritually superior to others. There was a major stigma associated with disability because disability was associated with sin.
For the people gathered in the home of Peter and Andrew that day, it was all about them. Those of us who are long-time church attenders are especially vulnerable to this line of thinking. We have an idea in our mind of how church should be… and have great difficulty tolerating any change in the way we do things, especially on Sunday morning. We’re at risk of becoming resentful because we fear the presence of newcomers with disabilities may detract from our church experience. Here’s the good news…we’re not cutting a hole in the roof of the sanctuary to help you welcome lots of new kids and families. You may see some kids who fidget more or talk more than the kids you’re accustomed to.
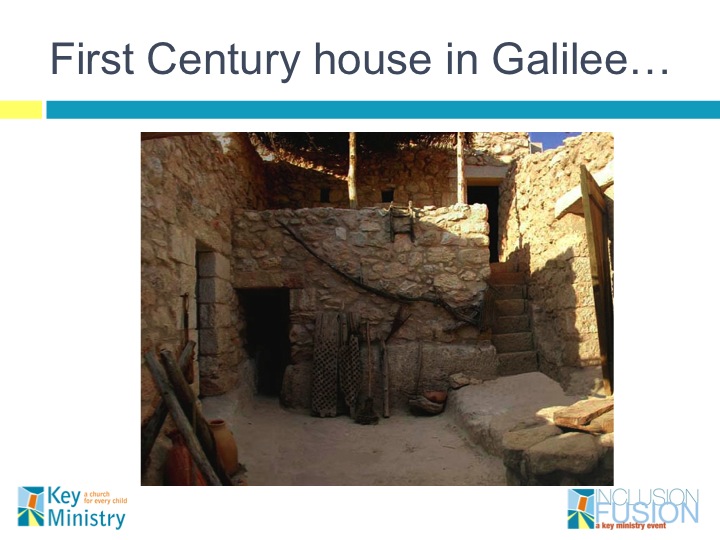
Another observation: the friends of the man who was paralyzed were willing to think “outside the box” to get their friend in front of Jesus. Here’s a picture of a reconstructed house from the first century in Israel. Typically, such a house would have one larger room (the size of a living room or family room today) and maybe one smaller room that would be entered through an open courtyard. There would be steps to the roof, where families slept when the weather became intolerably hot, and where women worked during the day while men were in the fields or tending their craft.
They get to the courtyard, where late arrivals were likely packed in hoping to catch part of what Jesus had to say. They see there’s no room, and they head for the roof. Let’s look at what they DIDN’T do…
They didn’t procrastinate or assume that Jesus would still be there the following day or week, despite that being a reasonable conclusion. After all, Capernaum was Jesus’ base of operations in Galilee. He’d healed there before… recall the story of Peter’s mother-and they may have easily rationalized they could come back at some other time. I can tell you that there are times as a follower of Jesus that I’ve made up excuses for not sharing my faith when I was uncomfortable. But Scripture teaches that tomorrow is promised to no one…a reality that the friends in the story clearly grasped.
They didn’t wimp out when they got up on the roof. In first century homes, there would be large wooden beams supporting the roof with smaller branches and twigs molded together in dried mud to form a covering for the spaces between the beams with a tile covering laid over the top so the roof might be occupied. They had to figure out where Jesus was in the room, pull up the right tiles, and knock out at least a 3’ X 6” opening between the beams near to where Jesus was seated. They had to work quickly, because where do you think the dried mud and branches would land while they were doing this? Probably on top of Jesus and the folks seated in the first couple of rows!
I wonder if the friends ever considered the possibility their actions might offend Jesus? I’d probably be a little unsettled if chunks of roof start falling on me while I’m speaking here with you. Scripture gives us no indication this action bothered Jesus. He noticed their faith…especially the faith of the man with paralysis.
They didn’t worry about the price for knocking a huge hole in the roof. I’m sure there was a significant expense involved in repairing a large hole in the roof of a private home. They could have been arrested. They were exposing themselves to ridicule from others in their community. Yet they cared enough about their friend that they were willing to take a chance.
One final observation about the story…the “friends” who went about the process of getting their friend to Jesus had no special qualifications aside from their willingness to serve. These weren’t religious professionals…just “ordinary” guys. Where in the Bible does it say that the work of sharing the Gospel and making disciples is reserved for ordained clergy and paid church staff? Romans 12:3-8 points out that every member of the “body” has gifts. USE THEM!
Let’s look back at the story…and compare ourselves to the friends on the roof…
We in the church know who Jesus is, yet where’s OUR urgency to get our friends and neighbors into the presence of Jesus?
We’re unwilling to step beyond our comfort zones to bring others to Jesus
AND…We’re afraid to take chances on behalf of those who need Jesus.
When was the last time you took a chance in order to introduce a friend or a neighbor to Jesus? After all, we understand the stakes to be a lot higher. The friends were seeking to relieve their friend from the burden of ten or twenty years of paralysis. We who call ourselves Christians know the stakes are MUCH greater. Eternity is on the line!
So…what do we do with this?
I’ll pledge that our team at Key Ministry will be available to your pastors, staff and volunteers to help you welcome and minister to any kids and families who come your way with disabilities that interfere with their ability to “do church”.
But what about you?
This initiative won’t work if you expect your church leadership to develop some model program to take care of kids with disabilities and their families. Tossing a check in the collection plate doesn’t absolve you of the responsibility to use your time and talents to build the Kingdom. This ministry is not a spectator sport!
You don’t need your church to launch a program to watch the neighbor’s kids so they can enjoy a night out together. You don’t need a program to offer to do kid pickup when your neighbor is stuck at the doctor. You can advocate for kids and families with disabilities in the juvenile court or social service systems. You could take the siblings of a kid with a disability to the football game next Friday…they may never get to go if their brother or sister can’t tolerate the crush of people, the noise of the crowd or the sound of the band. Your willingness to help neighbors with kids with disabilities may spark conversation about why your faith leads you to help. You may be the only Bible your neighbors get to read!
If you’d like to bring a family here with a child who might need a little extra help, call or e-mail Michelle…so your church will be prepared with a warm welcome.
If God’s positioned you where you come across lots of kids and families with conditions that may make it hard for them to “do church”, look for openings for spiritual conversations. When I meet families who have had negative church experiences, I offer to help connect them to a church where they’ll be welcomed.
Regardless of where you live or work, you’re positioned to influence other people as a representative of Christ. If you’ve experienced joy and comfort through your faith in Christ and value your experience being a part of this church, pray that God would open your eyes to people in your midst who need to be brought into the presence of Jesus and embolden you to extend the invitation to join everyone here at church. Like the man with paralysis…your friends and neighbors are depending on you to introduce them to Jesus.
Key Ministry’s mission is to help churches reach families affected by disability by providing FREE resources to pastors, volunteers, and individuals who wish to create an inclusive ministry environment. We have designed our Key Catalog to create fun opportunities for our ministry supporters to join in our mission through supporting a variety of gift options. Click here to check it out! For a sixty second summary of what Key Ministry does, watch the video below…
I’ll be heading down to Orlando next week for the American Academy of Child and Adolescent Psychiatry meetings…which brought to mind one of the leading lights of the disability ministry movement-Marie Kuck.
Marie is Co-Founder of Nathaniel’s Hope, a rapidly growing national ministry dedicated to sharing hope and encouragement with kids with special needs (VIP Kids) and their families, as well as educating and equipping local churches with tools and opportunities so that even the most inexperienced people can “be a a buddy” and reach out and minister to these families.
Nathaniel’s Hope has developed many programs to assist families, including a growing respite program called Buddy Break. Buddy Break is a free kids/respite program done in partnership with local churches that provides a free “break” for caregivers of kids with special needs. Marie and her husband (Tim) hope to build a national network of 1,000 churches to support VIP families with respite care. Other programs offered by Nathaniel’s Hope include Caroling for Kids, a National VIP Birthday Club, Keep ‘m Smiling, Hall of Hope, and an Online Resource Center. Last June, Nathaniel’s Hope hosted their 11th annual Make ‘m Smile festival at Lake Eola in downtown Orlando to honor and celebrate VIP kids, hosting over 10,000 people…including 1,500 VIP kids!
In Marie’s presentation from Inclusion Fusion 2012, she shares creative ways that churches…and the most fearful, inexperienced volunteer in the church-can serve kids with special needs and their families using fun, meaningful outreach opportunities. Nathaniel’s Hope has engaged thousands of “green” volunteers thru their annual Make ‘m Smile festival, Christmas Outreach and respite care program.
Our Key Ministry website is a resource through which church staff, volunteers, family members and caregivers can register for upcoming training events, request access to our library of downloadable ministry resources, contact our staff with training or consultation requests, access the content of our official ministry blog, or contribute their time, talent and treasure to the expansion of God’s Kingdom through the work of Key Ministry. In addition to our downloadable resources, those who register for our resource kit can view any presentation from our Inclusion Fusion Disability Ministry Web Summits “on-demand”. All of these resources are made available free of charge. Check out our website today!
Welcome to the seventh installment of our Fall 2013 blog series: Trauma and Kids…A Primer for Pastors, Church Staff and Parents. Today, we’ll look at the specific criteria for the syndrome we describe as Post-Traumatic Stress Disorder (PTSD).
Not all trauma leads to the development of Post-Traumatic Stress Disorder (PTSD).
When we use the term PTSD, we refer to a clinical syndrome resulting from exposure to actual (or threatened death), serious injury or sexual violence that…
is directly experienced
is witnessed, in person, the event(s) as it occurred to others
follows learning the event(s) occurred to a close family member or friend
occurs after experiencing repeated or extreme exposure to aversive details of traumatic events
PTSD is characterized by “intrusion symptoms” associated with the traumatic event, beginning after the traumatic event, including…
recurrent, involuntary and intrusive distressing memories
recurrent, distressing dreams
flashbacks (dissociative reactions in which the person responds as if the traumatic event is recurring
intense, prolonged psychological distress, or marked physiologic reaction upon exposure to internal or external cues associated with the event
PTSD is also characterized by persistent avoidance of stimuli associated with the traumatic event, including distressing thoughts, memories, feelings and distressing reminders of the event.
Children and adults with PTSD experience negative alterations in cognition and mood associated with the traumatic event, including at least two of the following symptoms…
inability to remember some important aspect of the traumatic event
persistent, exaggerated negative beliefs or expectations about oneself, others or the world
distorted cognitions about the cause(s) of the traumatic event, leading to self-blame
persistent, negative emotional states (fear, horror, anger, guilt, shame)
markedly diminished interest or participation in significant activities
detachment or estrangement from others
persistent inability to experience positive emotions
Persons with PTSD experience marked increases in arousal and reactivity associated with the traumatic event, as characterized by two or more of the following…
verbal and/or physical aggression toward people or objects
reckless, self-destructive behavior
hypervigilance
exaggerated startle response
difficulties with concentration
disturbed sleep
By definition, symptoms must persist for more than one month following the traumatic event in question and result in significant functional impairment.
Developmental regression is common in children with PTSD. Young children are more likely to manifest re-experiencing symptoms through play that refers directly or symbolically to the traumatic event. Persons with PTSD are 80% more likely than those without PTSD to have at least one or more “comorbid” disorders…kids with PTSD are more likely to have Oppositional Defiant Disorder and Separation Anxiety Disorder, males with PTSD are more likely to have concomitant substance use disorders and Conduct Disorder, with depressive, bipolar, anxiety and substance use disorders occurring more commonly among adults with PTSD.
Confused about all the changes in diagnostic terminology for kids with mental heath disorders? Key Ministry has a resource page summarizing our recent blog series examining the impact of the DSM-5 on kids with mental health disorders. Click this link for summary articles describing the changes in diagnostic criteria for conditions common among children and teens, along with links to other helpful resources!
I’m looking forward to meeting old and new friends this coming Sunday, October 20th at St. Mark’s United Methodist Church in Findlay, Ohio!
I’m honored by the opportunity to share the message at both Sunday morning worship services…the 8:45 AM service offers traditional worship with choir, organ, and piano in the church sanctuary, while “The Gathering” at 11:15 AM in “The Dock” is a casual, fresh, contemporary worship experience with a band and multimedia. I’ll be teaching from Mark 2:1-12 on the topic…The Mission Field Next Door.
Between the two worship services, I’ll be doing a presentation on “The 3 A’s”…ADHD, Anxiety and Aspberger’s Disorder: Overcoming Barriers to Spiritual Growth in Kids at St. Mark’s Fellowship Hall. We’ll talk about the functional impairments associated with ADHD, anxiety disorders and Asperger’s Disorder in children and teens, and share practical ideas for addressing the challenges each condition poses to “doing church” for the affected kids and their families. Everyone is welcome!
For a preview, here are the slides for our “3 A’s ” presentation…or if you prefer, you can download the slides here.
Our Key Ministry website is a resource through which church staff, volunteers, family members and caregivers can register for upcoming training events, request access to our library of downloadable ministry resources, contact our staff with training or consultation requests, access the content of our official ministry blog, or contribute their time, talent and treasure to the expansion of God’s Kingdom through the work of Key Ministry. In addition to our downloadable resources, those who register for our resource kit can view any presentation from our Inclusion Fusion Disability Ministry Web Summits “on-demand”. All of these resources are made available free of charge. Check out our website today!
We’re taking a week off from our Sunday night Faces of the Movement series. Instead, we’ll look at the complexity of problems facing America’s system of mental health care and preview a series we plan to run in 2014 examining in more depth the challenges families face in obtaining effective mental health care for their children and teens.
Lots of media attention has been devoted to the failings of our mental system in the aftermath of the mass shootings (Congresswoman Gabrielle Giffords, the Aurora theater massacre, Newtown, Washington Navy Yards) perpetrated by individuals with poorly treated or untreated mental illness.
The reality is that our mental health system fails millions of families in less spectacular ways on a daily basis.
The system is so dysfunctional, figuring out where to start can be an overwhelming intellectual exercise…not unlike the challenge I sometimes face when families bring kids with extremely complicated histories to our practice.
If we expect churches to do a better job of ministry with families impacted by mental illness, some awareness of the struggles families face in finding good care may be helpful. Having served in many different capacities in the system…as a child and adolescent psychiatrist in private practice, as Medical Director of a large, inner city children’s mental health center, as a consultant for our university hospital’s privately owned insurance company, as an investigator on several Federally-funded clinical research studies, as the Chairman of the Private Practice committee for my national specialty society, as Clinical Director of a large residential treatment center for teens and as the Board Chairman of our county’s community mental health center, here’s a formulation as to why our mental health system in the U.S. is failing so many of the families it was created to serve.
We don’t have a good understanding of the underlying brain and nervous system pathology foundational to specific mental illnesses, much less anything other than a rudimentary understanding of how environment impacts genetic expression in mental illness. The National Institute of Mental Health has launched its’ Research Domain Criteria initiative to stimulate the science necessary to better delineate the underlying causes of mental illness. The downside of the initiative is that in an era characterized by an emphasis upon “evidence-based medicine”, we’ll have very little new evidence to guide our treatments under the recently-released DSM-5 diagnostic system.
We don’t have the tools to accurately predict who among our population suffering from mental illness or psychopathy is most at risk of committing severe acts of violence, or to predict with any certainty who may act upon suicidal thoughts.
We have three systems of mental health care, with flaws inherent in each. Our public mental health system offers the broadest range of services at low or no cost to families below or near the poverty line, but is difficult to access and prohibitively expensive for middle class families who fail to qualify for large, sliding scale discounts. Commercial insurance pays for brief hospital stays, a limited number of outpatient visits with clinicians willing to massively discount their services and brief medication visits with psychiatrists disincentivised from scheduling longer appointments. Concierge practices offer rapid access to highly qualified clinicians, but generally provide a limited range of services and are prohibitively expensive for many families in need of more frequent or intensive care.
Mental health services are often very difficult to access when they’re needed. Many insurance websites fail to indicate when practitioners are closed to new patients. Waits for a psychiatrist in many cities are measured in months. Appointments are scheduled at times of the day more convenient for clinicians and institutions than for patients, requiring that parents miss work and kids miss school. I was teaching at a local children’s hospital a couple of months ago and was quite surprised to see the waiting room in the child psychiatry clinic empty shortly after 5:00 PM, when kids and families are generally most available for appointments on weekdays. Insufficient incentives exist for clinics to become more “consumer-friendly”.
Our methods of paying for mental health care greatly contribute to the overall dysfunction in the system. Psychiatrists can earn much more money for running an “assembly line” of patients through brief medication appointments than by spending time on lengthier evaluations. A colleague in my office works full-time at our local community mental health center. The center needed to hire two full-time nurses (and foot the bill for salaries and benefits) simply to fight with managed Medicaid plans and commercial insurers so that patients of the three psychiatrists can fill prescriptions written during their appointments. While patients wait weeks and months for appointments, clinicians spend large chunks of time completing the reams of paperwork necessary to survive Medicaid audits. Rates of reimbursement paid by the state to community mental health centers skyrocket to reimburse for the overhead costs connected to paperwork completion.
The geographic distribution of our most highly trained mental health professionals is highly uneven. The vast preponderance of child and adolescent psychiatrists practice in large, urban areas, heavily concentrated on the coasts. Access to specialized mental health services may be very limited in rural areas across the heartland.
Mental health services for special populations are in extremely short supply. Shortages of child psychiatrists and geriatric psychiatrists are especially acute. Families struggle to find qualified mental health care for adults with intellectual disabilities, geriatric patients with concomitant medical illness, or children and teens with inappropriate sexual behaviors.
Major obstacles exist to care coordination with other service providers or service systems. Time spent coordinating treatment with clinicians from other practices, school officials, and primary care physicians is almost never reimbursed. Uncompensated time in care coordination doesn’t count toward required productivity quotas for staff employed by clinics or large institutions.
We persist in employing an acute care medical model that has demonstrably failed in serving the chronically mentally ill. In our area, the average length of a hospital stay is four days. The moment a patient no longer has an active suicidal or homicidal plan discharge is mandated by insurance companies, before most medication response can be adequately assessed. Patients covered by private insurance have difficulty accessing the continuum of care they need following an acute crisis.
Great inconsistencies are present in the quality of available mental health services. This is especially true with non-medical mental health professionals, where less uniformity exists in training and supervision requirements.
We spend much of our resources seeking to address the consequences to individuals living in toxic environments in a declining social system. We can’t expect counseling or pills to help when kids are living in homes where they’re physically or sexually abused, witnessing ongoing domestic violence or neglected by chemically dependent parents or caregivers. Mental health services tend not to be successful when kids are suffering the consequences of the maladaptive choices of parents seeking to fill the emptiness in their lives at the expense of their families.
We’ll look at this topic in more detail in a blog series during the first quarter of next year. Given the tidal wave of change approaching the healthcare system in general, the shape of our mental heath service delivery systems in the next few years is anything but certain.
Photo courtesy of the Washington Post
***********************************************************************************************************
Confused about all the changes in diagnostic terminology for kids with mental heath disorders? Key Ministry has a resource page summarizing our recent blog series examining the impact of the DSM-5 on kids with mental health disorders. Click this link for summary articles describing the changes in diagnostic criteria for conditions common among children and teens, along with links to other helpful resources!
This weekend, Katie Wetherbee will be doing two, two hour “Half Track” presentations at the Group KidMin (Children’s Ministry) Conference in Columbus, Ohio. Her presentations this weekend will focus upon how common disabilities affect faith development and cause obstacles for church attendance, ways to communicate effectively with parents of children with special needs, easy-to-implement strategies for welcoming and teaching kids with special needs, including behavior management, classroom culture and curriculum modifications.
Katie’s presentations this weekend will also mark the end of a nearly eight-year long formal relationship with Key Ministry. Katie began her service to Key Ministry in 2005 as one of our first two Board members from outside the church where our ministry originated. She did a fabulous job putting together our first CD-ROM toolkit, and is responsible for many of the fabulous resources currently available for free on the Key Ministry website. She was indispensable in the development of Inclusion Fusion.
Katie has received the opportunity to work on a very special project with our good friend Jolene Philo. Katie and Jolene have signed a book contract with Kragel Publications to author Every Child Welcome: A Menu of Strategies for Including Kids with Special Needs at Church. Jolene has a great description of the upcoming book on her blog. Much of the practical advice Katie has shared over the years with church staff and volunteers in Key Ministry-sponsored trainings will be available to a wider audience through the book she’s co-authoring with Jolene.
To honor Katie and her contributions to the ministry over the past eight years, we thought we’d share her presentation from last year’s Inclusion Fusion Web Summit… Sticks and Stones, Clicks and Phones: Solutions for Preventing Bullying at Church.
Here’s a description of Katie’s talk…
It has become a national public health crisis keeping over 160,000 children home from school every day.
Adults need to be aware of the signs and symptoms of this issue:
Sudden changes in appetite
Gastrointestinal distress
Chronic headaches
Loss of eye contact
Poor posture
Decreased communication with parents and peers
Increase of nervous habits such as tics or nail biting
It’s not autism. It’s not a virus or an environmental issue. So what is this insidious threat?
Bullying.
And unfortunately, bullying is not only happening in schools, but in neighborhoods and extracurricular activities as well. Sadly, children with special needs are often targeted by bullies at a much higher rate than their typically developing peers. This causes a great impediment to their learning and their opportunities to make and keep friends. Students report that often, adults don’t know about the instances of bullying. In addition, peers join in or ignore the bullying as it occurs.
Research tells us that bullying is largely about social power…attaining it and keeping it. While we might think of a bully as a large, tough caricature, children who engage in this behavior are very likely to look just like anyone else. Many times, these individuals are in the middle of the social power structure and are trying to gain more recognition from those they perceive as having more control. To accomplish this, children who bully others exclude, start rumors or tease their targets. When others join in or laugh, the “bully” has been recognized as a leader and therefore, has power. This cycle can be difficult to break, both for the child who is bullied AND for the child who is bullying others.
In her presentation for Inclusion Fusion 2012, Katie tackled the issue of bullying…and focused on bullying prevention. Pastors, KidMin leaders and volunteers need to know how to proactively prevent bullying, because sadly, this kind of behavior can—and does—occur in churches, too. In this presentation, she shared some practical strategies that can change the social culture of Sunday mornings.
Wouldn’t it be wonderful if what we accomplish at church could change the culture of schools and neighborhoods as well?
On behalf of our Board and staff…Thanks Katie for all you did to advance the mission of Key Ministry! We look forward to, and will be praying for your future ministry adventures!
Our Key Ministry website is a resource through which church staff, volunteers, family members and caregivers can register for upcoming training events, request access to our library of downloadable ministry resources, contact our staff with training or consultation requests, access the content of our official ministry blog, or contribute their time, talent and treasure to the expansion of God’s Kingdom through the work of Key Ministry. In addition to our downloadable resources, those who register for our resource kit can view any presentation from our Inclusion Fusion Disability Ministry Web Summits “on-demand”. All of these resources are made available free of charge. Check out our website today!

 For the first time in several years I had the opportunity to attend the American Academy of Child and Adolescent Psychiatry’s Annual Meeting, held this year in one of my favorite cities…Orlando, Florida.
For the first time in several years I had the opportunity to attend the American Academy of Child and Adolescent Psychiatry’s Annual Meeting, held this year in one of my favorite cities…Orlando, Florida. One of the challenges we face as clinicians when treating kids with depression is accurately describing to parents the additional benefits of combining cognitive-behavioral therapy (CBT) with medication. A study by Dr. Manesh Aligeti and colleagues at UT Southwestern Medical School looked at the benefits of CBT for relapse prevention in a sample of 8-17 year-old patients (N=144) who had been positive responders to fluoxetine. The only impact the CBT appeared to have on medication management involved the use of lower doses of fluoxetine among the kids who were also receiving therapy. Examining the same patient sample, Dr. Graham Emslie found that kids receiving CBT in addition to medication had a significantly lower risk of relapse than those receiving medication alone during the 30-week continuation treatment period of the study. The estimated probability of relapse was 7.5% among kids receiving medication and CBT vs. 28% among kids receiving CBT alone.
One of the challenges we face as clinicians when treating kids with depression is accurately describing to parents the additional benefits of combining cognitive-behavioral therapy (CBT) with medication. A study by Dr. Manesh Aligeti and colleagues at UT Southwestern Medical School looked at the benefits of CBT for relapse prevention in a sample of 8-17 year-old patients (N=144) who had been positive responders to fluoxetine. The only impact the CBT appeared to have on medication management involved the use of lower doses of fluoxetine among the kids who were also receiving therapy. Examining the same patient sample, Dr. Graham Emslie found that kids receiving CBT in addition to medication had a significantly lower risk of relapse than those receiving medication alone during the 30-week continuation treatment period of the study. The estimated probability of relapse was 7.5% among kids receiving medication and CBT vs. 28% among kids receiving CBT alone. Dr. Linmarie Sikich and her team at the University of North Carolina sought to determine the tolerability and efficacy of extended treatment with intranasal oxytocin (a pituitary hormone referred to by some as the “bonding hormone”) as a supplemental treatment for children and adolescents with an autism spectrum disorder. Measures of social reciprocity and social functioning showed improvement in the oxytocin group vs the placebo group. The improvements persisted and were more noticable with extended (16 week) treatment. There was no difference in adverse effects of the treatment group versus children and teens who received placebo. Oxytocin appears to have been well tolerated by most children over 16 weeks of sustained treatment. The hormone appeared to reduce irritability and improve some aspects of social functioning in a sample of 3-17 year-old patients with autism spectrum disorders.
Dr. Linmarie Sikich and her team at the University of North Carolina sought to determine the tolerability and efficacy of extended treatment with intranasal oxytocin (a pituitary hormone referred to by some as the “bonding hormone”) as a supplemental treatment for children and adolescents with an autism spectrum disorder. Measures of social reciprocity and social functioning showed improvement in the oxytocin group vs the placebo group. The improvements persisted and were more noticable with extended (16 week) treatment. There was no difference in adverse effects of the treatment group versus children and teens who received placebo. Oxytocin appears to have been well tolerated by most children over 16 weeks of sustained treatment. The hormone appeared to reduce irritability and improve some aspects of social functioning in a sample of 3-17 year-old patients with autism spectrum disorders. Finally, in an issue that hits close to home and has been a long-term concern of mine, a team from The Ohio State University compared polypharmacy patterns and rates over time among kids in foster care (FC), kids with disabilities (ABD), and low income kids (CFC) who qualified for Medicaid. Kids ages 17 years and younger who were continuously enrolled in Ohio Medicaid for a 1-year period and prescribed at least one psychotropic medication (antidepressants, antipsychotics mood stabilizers, stimulants, alpha-agonists and anxiolytics) during fiscal years 2002 (n = 26,252) through 2008 (n = 50,319) were selected. Polypharmacy was defined as ≥ 3 medications and multi-class polypharmacy as ≥ 3 medications from different drug classes. Both types of polypharmacy increased across all three eligibility groups. Polypharmacy increased from 8.8% to 11.5% for CFC youth, from 18.0% to 24.9% for ABD youth and from 19.8% to 27.3% for FC youth. Combinations that increased the most were two or more antipsychotics, two or more stimulants, and antipsychotics with stimulants and other psychotropic medications excluding antidepressants. Highest rates of polypharmacy were noted among youth in foster care.
Finally, in an issue that hits close to home and has been a long-term concern of mine, a team from The Ohio State University compared polypharmacy patterns and rates over time among kids in foster care (FC), kids with disabilities (ABD), and low income kids (CFC) who qualified for Medicaid. Kids ages 17 years and younger who were continuously enrolled in Ohio Medicaid for a 1-year period and prescribed at least one psychotropic medication (antidepressants, antipsychotics mood stabilizers, stimulants, alpha-agonists and anxiolytics) during fiscal years 2002 (n = 26,252) through 2008 (n = 50,319) were selected. Polypharmacy was defined as ≥ 3 medications and multi-class polypharmacy as ≥ 3 medications from different drug classes. Both types of polypharmacy increased across all three eligibility groups. Polypharmacy increased from 8.8% to 11.5% for CFC youth, from 18.0% to 24.9% for ABD youth and from 19.8% to 27.3% for FC youth. Combinations that increased the most were two or more antipsychotics, two or more stimulants, and antipsychotics with stimulants and other psychotropic medications excluding antidepressants. Highest rates of polypharmacy were noted among youth in foster care. AACAP Resource Centers empower consumers through patient education. Each AACAP Resource Center contains consumer-friendly definitions, answers to frequently asked questions, clinical resources, expert videos, and abstracts from the JAACAP, Scientific Proceedings and Facts for Families relevant to each disorder. Check out AACAP Resource Centers on ADHD, anxiety disorders, autism, bipolar disorder, bullying, child abuse, Conduct Disorder, depression, disaster, military families, Oppositional Defiant Disorder and substance use by clicking here.
AACAP Resource Centers empower consumers through patient education. Each AACAP Resource Center contains consumer-friendly definitions, answers to frequently asked questions, clinical resources, expert videos, and abstracts from the JAACAP, Scientific Proceedings and Facts for Families relevant to each disorder. Check out AACAP Resource Centers on ADHD, anxiety disorders, autism, bipolar disorder, bullying, child abuse, Conduct Disorder, depression, disaster, military families, Oppositional Defiant Disorder and substance use by clicking here.